| |
The Foreskin, Circumcision
and Sexuality
"Like being hugged by the Venus de Milo"
The foreskin in sex
Structure of the foreskin
It has been known since antiquity that the
foreskin gives pleasure, and only forgotten in the US in
the last century or so.
Central to Intactivist claims about foreskin function in
sex is the work of Taylor et
al., demonstrating that the foreskin itself is richly
innervated with Meissner corpuscles, which are sensitive
to light touch. They make the foreskin's sensitivity comparable
to that of the fingertips or the lips (but probably less than
that of the tip of the tongue or the eyelashes)
The ridged band now has
its own website, hosted
by its discoverer, Dr John Taylor.
|
... the type, not just the amount, of skin lost to
routine male circumcision is often overlooked.
Anatomically and physiologically, the skin of the
penis is designed to activate the male sexual reflex
mechanism. To perform this interesting function it is
richly endowed with smooth muscle fibres that cause
its upper, (sexual contact) surface to 'firm up' and
wrinkle - and become much more frictional - during
erection.
During vaginal intromission these conformational
changes in penile skin ensure stretching of ridged
band and reflex contraction of bulb muscles .
In short, the penile skin behaves in exactly the same
way, during erection, as scrotal skin. Almost
certainly, uniquely-structuresd penile and scrotal
skin play an important role in activating and
moderating erogenous sensation and sexual reflexes for
ejacuation. As far as I know, there is no female
equivalent.
In short, male circumcision completely alters the way
male sexual sensations and reflexes are generated
during vaginal intercourse.
- John Taylor
|
Meissner's corpuscles
J. Anat, June 2, 2021
Sensory innervation of the
human male prepuce: Meissner's corpuscles predominate
Yolanda García-Mesa, Jorge García-Piqueras, Ramón Cobo,
José Martín-Cruces, Iván Suazo, Olivia García-Suárez,
Jorge Feito, José A. Vega
Abstract
Meissner's corpuscles are the most abundant sensory
corpuscles in the glabrous skin of the male prepuce.
They are type I, rapidly
adapting, low-threshold mechanoreceptors, and
their function is linked to the expression of the
mechanoprotein piezo-type mechanosensitive ion channel
component 2 (PIEZO2). Stimulation
of genital Meissner's corpuscles gives rise to
sexual sensations. It
has been recently demonstrated that digital Meissner's
corpuscles, Meissner-like corpuscles, and genital end
bulbs have an endoneurium-like capsule surrounding
their neuronal elements; that is, the axon and glial
lamellar cells, and their axons, display PIEZO2
immunoreactivity. It is unknown whether this is also
the case for preputial Meissner's corpuscles.
Furthermore, the expression of certain proteins that
have been found in Meissner's corpuscles at other
anatomical locations, especially in the digits, has
not been investigated in preputial Meissner's
corpuscles. Here, we used immunohistochemistry to
investigate the expression of axonal (neurofilament,
neuron-specific enolase), glial (S100 protein, glial
fibrillary acidic protein, vimentin), endoneurial
(CD34), and perineurial (glucose transporter 1)
markers in the preputial and digital Meissner's
corpuscles of male participants aged between 5 and 23
years. Furthermore, we investigated the occurrence of
the mechanoprotein PIEZO2 in male preputial Meissner's
corpuscles. Human
male prepuce contains numerous Meissner's corpuscles,
which may be grouped or isolated and are regularly
distributed in the dermal papillae. Lamellar
glial cells display strong expression of S100 protein
and vimentin but lack expression of glial fibrillary
acidic protein. In addition, they show axonal PIEZO2
expression and have an endoneurial capsule, but no
perineurial. Our results indicate that human
male preputial Meissner's corpuscles share the
immunohistochemical profile of digital Meissner's
corpuscles, which is considered to be necessary for
mechanotransduction. These data strongly suggest that
the structure and function of Meissner's corpuscles are
independent of their anatomical location.
{In other words, they
are as sensitive as those of the fingertips..]
|
The role of the foreskin in intercourse
The movement of the foreskin is
unique. On the in-stroke of intercourse, considered from the
point of view of its stationary outer layer, the inner layer
rolls outward and applies itself to the vagina. The ridged band
engages with the internal ridges of the vagina. On the
out-stroke, that movement reverses. Depending on the various
dimensions and techniques used, there is considerable variation
from that basic pattern and the two sets of ridges may then rub
over each other like clothes on an old-fashioned washboard. That
might be painful for women if the foreskin were dry like the
circumcised penis. Instead, the effect is pleasurable.
First-person accounts
By men:
|
What happens with me is that during entry into the
vagina, the labia minora (inner vaginal lips) catches
the foreskin and retracts it behind the ridge of the
glans. That's where it stays until intercourse is
complete and the erection subsides. My partner tells
me that this is the normal course of events if the
foreskin does not retract on its' own when it becomes
erect. The labia minora are so shaped as to catch
under the edge of the foreskin, which is usually
partially retracted, and push it back. The exposed
glans is then exposed to the full friction of the
vaginal walls when thrusting.
|
This is one of the variations. The ridged band is in intimate
contact with the labia minora rather than the vaginal walls,
another kind of intimacy unavailable to the circumcised man.
Moderate stretching of the foreskin may also be pleasurable for
the man. This gives rise to the "balloon job" - inflating the
foreskin - possible only for an intact man. (Air should not be
forced down the urethra, and on no account should high-pressure
air supplies be used.)
|
European porn actor Mario Rossi:
Rossi: You know what? European girls know how to
suck the European c ck. They are soft and nice and
gentle and they know that. Because we're more
sensitive so we need a gentle treatment.
Adair: So you're saying American girls are too
rough?
Rossi: Yeah because if you're circumcised it means
you're not as sensitive and so the girls have to be
rough.
- from the film: "Georgia Adair - Self
Portrait"
|
|
AlterNet
April 15, 2008
Uncut is better I have proof
by ashkewoof
Uncut by birth, got cut at 18 because I was confused
that cut penises looked better.
I have tried to live without regret and I swore when
I got circumcised, I would never regret it.
I now live with that regret. I am reminded of this
regret every time I am intimate with a partner.
With my foreskin went a wonderful degree of
sensuality and sensitivity that I will never get back
and never knew I would miss until it was gone. I had a
whole lot of experience with a foreskin before I was
cut and a whole lot of experience without one after I
was cut.
I am in a very good position to speak on the subject
clearly since I have experienced both sides of the
issue for long periods of time.
I want to scream when I hear parents making the
choice to mutilate their child for cleanliness,
aesthetics or misplaced notions of health. With a few
necessary medical exceptions, this is barbarity and it
is mutilating your son in the most intimate of ways.
My penis was always clean, happy and wonderful. Now
part of it, a truly wonderful part of it is gone and
restoration will not bring it back.
Stop butchering your children and STOP making this
choice for them!
It should be illegal to do this to children. If they
want to do so later on their journey through this
life, when they are adults for whatever reason,
religious or otherwise, let them. No one should
mutilate children at an age especially when they can
not consent to it.
RE: Uncut is better I have proof
Posted by: Dr. P. Mooney on Apr 15, 2008 8:47 AM
I totally, agree with you. I too, have been on both
sides of this issue having my "child-hood operation"
at the age of 24 or 25 yrs. old. It was done for
medical reasons and had nothing to do with any of
the other reasons associated with having it done.
One does lose a lot of sensitivity removing the
foreskin. It offers many functions from protection
of the glans to lubrication of it. When the glans is
continually, exposed to the elements, it loses
sensitivity. I think all reasons for removing it
save, medically, are not worth mutilating a
functioning piece of anatomy.
|
|
...
I was cut as an adult (medical error), so I know the
difference. It would be a cliché to say "day and
night", so I should describe it like this: if
being intact is a milkshake, being cut is skimmed
milk; circumcision greatly reduces the "flavor" of
sex.
So you see, I can't regard circumcision as anything
but absolutely evil. As far as I am concerned, anyone
who performs a circumcision is even more depraved than
someone who would rape that same child.
-Rodrigo Girao on Huffington Post October 3, 2011
|
|
im 50 now at the age of 30 i decided to get
circumcised. since then i have no sensation
whatsoever. i am numb and there is no pleasure. i do
not enjoy masterbation like before and i do not enjoy
sexual intercourse ...
from someone who knows. don't do this to your babies
- meanmachinemarine on YouTube, 2009
|
|
I was intact until I was 19, and after some bad
medical advice I was circumcised. There is no
comparison in sensation - before I had an exquisitely
sensitive sexual organ. Now the sensation is nil. I
have erectile dysfunction and do not orgasm.
...
I wish every day I could go back and not make that
mistake. It has totally destroyed my life.
- Steve Bennett on MindofOwn, June 22, 2012
|
By women:
|
When I was younger I lived in Italy and the men I had
sex with were very vocal and ecstatic in their
lovemaking, and specifically in their orgasmic voice.
Back in the USA my boyfriends did not express sexual
pleasure the same way. They would kind of grunt, set
their jaw or say, "Oh God, I'm going to cum!" but -
not SING from the centers of their souls.
I thought that it was a cultural thing, that somehow
the Italians had learned to express themselves (like
some women learn to fake noises to thrill their
partner) and the American guys had conversly learned
to supress their expression of their feelings. At the
time I didn't make a connection, I thought it had to
do with Italian vs. American culture.
Then, years later, I had a British boyfriend who was
culturally much more like an American than like an
Italian, but when he came he sang and cried out - not
with a feminine voice, but with a passion that was
"feminine" only in as much as - in my American world -
women have it and men don't....
At that point I was able to see that it was not
Italians vs Americans, but Intact men vs circumcised
men. It was a very sad realization.
Although I will never know what they were actually
feeling - how it was different - I do know that what I
could see and hear and feel as an observer there
seemed to be a dramatic difference.
- S on Facebook, July 10, 2011
|
|
LILAC COLORED GLASSES
Ooh,
and here's the best part. Okay, girls who have done
it with a cut penis, hopefully you know what I
mean...you know right when the penis is going in,
there's almost like, a sharp sensation? Not, like,
ouch, knife sharp but more like...like how an orange
must feel when you stick a wooden juicer into the
middle of it? Well when the penis has foreskin, that
sensation isn't there. Entry feels a lot smoother
and to me that's much more enjoyable.
And
you know that drop of pre-ejaculate (pre cum in
laymen's terms)? Well when I was with circumcized
guys that was kind of like "ew, wipe it off" but
with foreskin that drop of fluid is preserved and
serves as a lubricant for the man. Know what that
means? No rawness or chafing after repeated
intercourse! Hooray!!
- a 26-year-old from
Pittsburgh living in Belgium
|
|
THE JOYS OF THE
UNCIRCUMCISED PENIS
I have never been with anyone who was uncircumcised
until I met my new boyfriend, and it's amazing. The
extra skin is like having an extra ridge there. When
I have children, I won't have the boys circumcised,
because I want their wives to be very happy. It's
almost like he has a cock ring on. You know those
condoms that have the big ridges on them? Well,
that's what it's like. Besides, a dick is a dick. It
just looks a little different. And my boyfriend's is
the perfect size. You usually don't remember how big
men's dick's are, but you remember the really small
ones. Girth matters and size and length matter.
Basically, I have to have a perfect dick. And now
I've got the length and the girth and a bonus I
didn't even know existed.
- Heidi Mark, Playboy's
Miss
July, 1995
|
|
The
foreskin
is my go-to guy when I'm lazy during BJ or handjobs!
It's the dick that strokes itself!
- dictaste on Dodson and Ross, April 8, 2010
|
|
My sons will NOT be cut! I think the increased sexual
pleasure far outweighs the rare risk of problems
(which still can be handled later in life if need be).
From the female point of view, my intact boyfriends
were MUCH, MUCH, MUCH! more sensitive during
intercourse, and neither had any problems with odor or
infection. One I was with for over 10 years, so I
certainly would have known.
When I discovered my current significant other was
uncircumcised, I felt I had hit the jackpot! Women who
are "afraid" of an uncircumcised man have no idea what
they are missing!
Sincerely,
Enlightened female in the US.
-Bargain shopper on Amazon.com, June 2, 2011
|
|
I
have two sons under three. Their father is cut, but
I persuaded him not to circumcise them. A previous
longtime boyfriend had been uncircumcised, and as a
woman with a narrow vaginal opening, the sex with
him, which had often been painful with others even
with lubricant, was much easier and kinder on my
body. (After giving birth, this was no longer an
issue :) ..
- newtrack on the Chronicle
of
Highr Education, June 23, 2010
|
|
... someone who was
probably done at birth, ...
and who has absolutely no idea what it's like to have
a foreskin. Or indeed any idea of what it's like from
a woman's point of view to put up with a
circumcised man pounding away for what seems like
hours, getting more and more sore. I've only
got a sample of two to go by, but the experience with
those two men was fundamentally different to those
where the men had all their equipment.
Sunday Morning in the Independent, May 7, 2011
|
|
A love letter to your uncircumcised dick
Dear boyfriend,
I love your dick.
I'm using a throwaway account
even though I have a throwaway account already,
because you know about my real throwaway account,
and I don't want you to think I'm some dick-obsessed
psycho. I feel like if you read this, you'd know it
was me, but you probably won't ask me, because
saying, "Hey, did you write a post on Reddit about
how much you love my dick?" is a weird thing to ask
someone, so I think I'm in the clear. But anyway, I
really need to write this. So, new throwaway, here
goes.
I love your dick.
I love giving you blowjobs.
I love having sex with you.
I love the way your dick looks when it's hard.
And I also love the way it looks when it's flaccid,
because guess what?
I love your foreskin.
Honestly, I do. Your dick is my favourite one I've
ever had the privilege of seeing. Not that I've seen
that many dicks in real life, but out all all the ones
I've seen, I like yours the best. I've told you that
before, but you shrugged it off because that's the
kind of thing that girls say to every single boyfriend
they have for reassurance. But it is the truth.
You don't believe me because girls aren't supposed to
like uncircumcised dicks. We're supposed to be grossed
out by them and not know what to do with them and
think you're some kind of weird-dicked freak. The
first time you pulled down your pants, you probably
expected me to be disappointed that you weren't cut,
like everyone else I've ever been with. You still try
to cover your dick whenever it's soft, with a blanket
after sex, or your hand when you get dressed. You
think it's embarrassing because when it's flaccid, you
cant just pull your foreskin back and make it look
cut.
But I love it. I love the slightly taboo nature of
your dick. I love how your foreskin is like some rare
and secret special thing that not everyone else has.
It's like a gift. I love how there's something raw
about having sex with you. How even when we're
"fucking" it still feels like "making love", because
it's like you're somehow closer to me (that might be
because I fucking love you, but I'm sure your dick
doesn't hurt either). I love how having sex with you
feels. So much. It literally turns me on to type this.
Physically (duh) and emotionally. You're the best
sexual partner I've ever had. It's somehow more
intimate to be with you than anyone else I've ever
been with.
One day I'm gonna just tell you to your face how much
I love your dick and how I masturbate thinking about
it and how it's literally become a fetish for me since
we started dating. I tell you everything, but goddamn,
it's hard to tell someone that something they think is
weird is the biggest turn on ever for you. But I'm
gonna tell you. Hopefully you won't think I'm too
crazy.
But for now, I'll just post this on reddit, and go
touch myself and think about you.
Sincerely,
Your dick-crazed girlfriend.
- oopsiloveyourdick on reddit, April 14, 2014
|
The effect of circumcision on sex
|
Int J Epidemiol. 2011 Jun 14.
[Epub ahead of print]
Male circumcision and sexual function in men and
women: a survey-based, cross-sectional study in
Denmark.
Frisch M, Lindholm M, Grønbæk M.
Abstract
BACKGROUND:
One-third of the world's men are circumcised, but
little is known about possible sexual consequences of
male circumcision. In Denmark (~5% circumcised), we
examined associations of male circumcision with a
range of sexual measures in both sexes.
METHODS:
Participants in a national health survey (n = 5552)
provided information about their own (men) or their
spouse's (women) circumcision status and details about
their sex lives. Logistic regression-derived odds
ratios (ORs) measured associations of circumcision
status with sexual experiences and current
difficulties with sexual desire, sexual needs
fulfilment and sexual functio ning.
RESULTS:
Age at first intercourse, perceived importance of a
good sex life and current sexual activity differed
little between circumcised and uncircumcised men or
between women with circumcised and uncircumcised
spouses. However, circumcised
men reported more partners and were
more likely to report frequent orgasm difficulties
after adjustment for potential confounding factors [11 vs 4%, OR(adj) = 3.26; 95%
confidence interval (CI) 1.42-7.47], and women with
circumcised spouses more often reported incomplete
sexual needs fulfilment (38 vs 28%, OR(adj) =
2.09; 95% CI 1.05-4.16) and frequent
sexual function difficulties overall (31 vs
22%, OR(adj) = 3.26; 95% CI 1.15-9.27), notably orgasm
difficulties (19 vs 14%, OR(adj) = 2.66; 95% CI
1.07-6.66) and dyspareunia [painful
intercourse] (12
vs 3%, OR(adj) = 8.45; 95% CI 3.01-23.74).
Findings were stable in several robustness analyses,
including one restricted to non-Jews and non-Moslems.
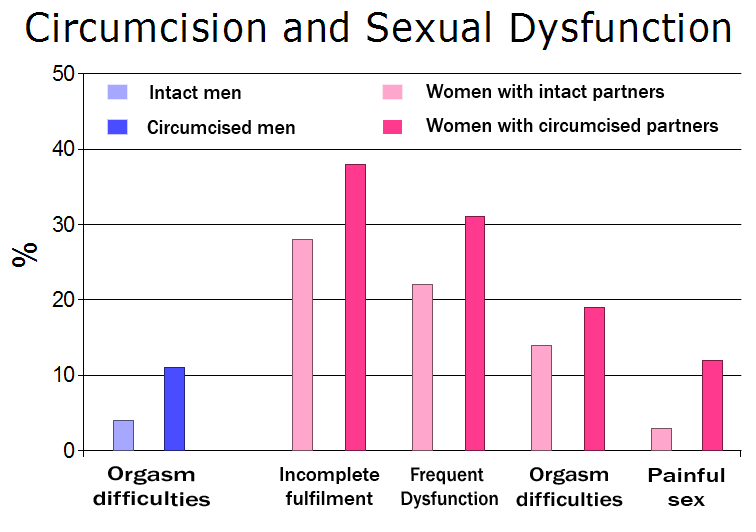
[Graph created
for this site based on the above data]
Conclusions
Our study shows hitherto unrecognized associations
between male circumcision and sexual difficulties in
both men and women. While confirmatory findings in
other settings are warranted, notably from areas where
neonatal circumcision is more common, our findings may
inform doctors and parents of baby boys for whom the
decision of whether or not to circumcise is not
dictated by religious or cultural traditions.
Additionally, since it appears from our study that
both men and women may have fewer sexual problems when
the man is uncircumcised, and because preputial
plasties may sometimes serve as suitable alternatives
to standard circumcision, our study may stimulate a
more conservative, tissue-preserving attitude in
situations where foreskin pathology requires surgical
intervention.
-
|
This study was attacked by, predictibly,
circumcision advocates Brian Morris, Jake Waskett and
Ronald Gray. Frisch as roundly defended it, saying inter
alia:
...
as these critics repeatedly refer to Morris’
pro-circumcision manifesto1 as their source
of knowledge, their objectivity must be questioned.
...
Morris et al. argue that our finding of considerably
higher rates of frequent orgasm difficulties in
(partially) circumcised than uncircumcised Danish men
(11 vs 4%, OR 3.26) may not apply in countries where
circumcision means complete amputation of the
foreskin. This may well be the case. If partial
amputation of the foreskin truly entails frequent
orgasm difficulties in a noticeable proportion of men
(as experienced by 11% of circumcised men in our
study), comparable proportions may well be larger and
associated ORs even higher in countries where
circumcised men experience greater tissue loss due to
more extensive circumcision procedures. Obviously,
more data are needed from rigorous studies using
carefully constructed questionnaires. ...
Morris et al. should be commended for their creative
attempt to dismiss the higher prevalence of frequent
dyspareunia in women with circumcised (12%) than
uncircumcised (4%) spouses (ORs between 4.17 and
9.00). They suggest that Danish women with circumcised
spouses may be so psychologically troubled by the
shape of their spouse's penis that it might result in
painful intercourse. A more plausible explanation
would be that reduced penile
sensitivity may raise the need among some
circumcised men for more vigorous and, to some
women, painful stimulation during intercourse in
their pursuit of orgasm.
Two of the authors, Morris and Waskett, both
internationally recognized circumcision activists,6,7
forget to declare their conflicts of interest. Even in
situations that are out of context, Morris promotes
himself as a neutral ‘authority on the extensive
medical benefits of this simple surgical procedure',8
whereas at the same time he argues that neonatal male
circumcision 'should
be made compulsory' and that 'any parents not
wanting their child circumcised really need good
talking to'.9
...
Like in critical letters to the editor following
other recent studies that failed to support their
agenda,10–12 Morris et al. air a series of
harsh criticisms against our study. As seen, however,
the points raised are not well founded. It
seems that the main purpose, as with prior letters,
is to be able in future writings to refer to our
study as an 'outlier study' or one that has been
'debunked', 'rejected by credible researchers' or
'shown wrong in subsequent proper statistical
analysis'. This in spite of the fact that our
study was carried out using conventional
epidemiological and statistical methods, underwent
peer-review and was published in an international
top-ranking epidemiology journal.
I would like to thank the IJE editors for
withstanding the pressure from
one particularly discourteous and bullying reviewer
who went to extremes to prevent our study from
being published. After the paper's
online publication, I have received emails from
colleagues around the world who felt our contribution
was useful and potentially important. One colleague
informed me that the angry
reviewer was the first author of the above letter to
the editor. In an email, Morris had called
people on his mailing list to arms against our study,
openly admitting that he was the reviewer and that he
had tried to get the paper rejected. To inspire his
followers, Morris had attached his two exceedingly
long and aggressive reviews of our paper (12 858 words
and 5291 words, respectively), calling for critical
letters in abundance to the IJE editors. Breaking
unwritten confidentiality and courtesy rules of the
peer-review process, Morris distributed his slandering
criticism of our study to people working for the same
cause. Rather than resorting to such selective
distribution among friends, Morris should make both
reviews freely available on the internet by posting
them in their entirety on his pro circumcision
homepage (www.circinfo.net). Alternatively, interested
readers should feel free to request them from me at
the e-mail address above. Despite poorly
founded
criticisms and attempts
at
obstruction our findings suggest that male circumcision may be associated
with hitherto unappreciated negative sexual
consequences in a non-trivial proportion of men and
women.
|
It is repeatedly claimed that
"Circumcision has no effect on sexual function."
For example in "Babywatching",
Desmond Morris says circumcision "has no effect, one way or the
other, on the sexual performance of the adult male." Books for
young people, especially, protest too much, such as the British
Family Planning Association's "How Sex Works": "Whether you have
a foreskin or not will not affect your sexual health in the
future."
This claim flies in the face of common sense. The foreskin is
ideally placed to both give and receive sexual stimulation, and
it would be extraordinary if it did not.
This study shows that the foreskin is the most touch-sensitive
part of the penis:
|
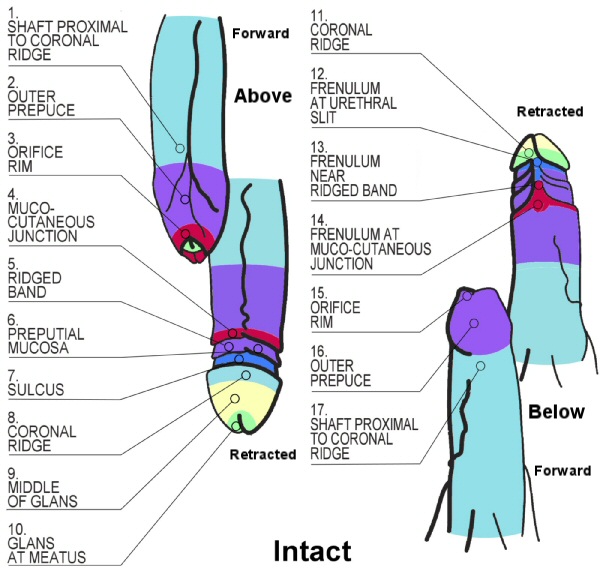
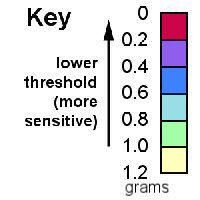
Fine-touch
pressure
thresholds in the adult penis
Morris
L. Sorrells, James L. Snyder, Mark D. Reiss,
Christopher Eden, Marilyn F. Milos, Norma Wilcox,
Robert S. Van Howe
BJU International 99 (4), 864-869 (British
Journal of Urology International,
Volume 99 Issue 4 Page 864 - April 2007)
Circumcision removes the most sensitive part of a
man's penis. Sorrells and others enlisted 159 men
from the San Francisco Bay area, 91 of them
circumcised, and conducted touch-sensitivity tests,
using instruments
that press with calibrated hairs, on 11 or 17
different places on their penises. The men could not
see where they were being touched.
Larger image
Larger image
|
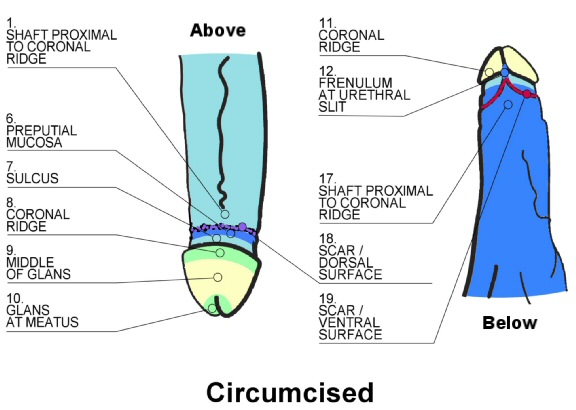
They
found that the most sensitive part of a
circumcised penis is on the scar in the
middle underneath (19). But several places
on the foreskin (3, 4, 13, 14) are more
sensitive than that. The glans (8, 9, 10 11)
is the least sensitive part of the
penis, contrary to a
common claim, but where it is covered
by the foreskin (8, 9,11), the glans of the
intact penis is more sensitive than the
circumcised.
|
 |
Larger
image
The
experimenters took into account the men's age, type
of underwear worn, time since last ejaculation,
ethnicity, country of birth, and level of education.
|
This study was of course criticised because its authors are
Intactivists, but carrying out such studies take considerable
dedication, so few who conduct them can be completely without
involvement, and the data is there to be checked for accuracy.
(Just getting ethical approval is a major hurdle, even though
circumcision itself has never had ethical approval.) A critique
by Morris and Waskett succeeded in
nullifying the data by the simple expedient of removing the
measurements from the foreskin "since these are ... not present
on a circumcised penis". Well, duh. They invoke "the Bonferroni
method to correct for multiple comparisons" but that is not
appropriate here.
This result has been confirmed - at least for the glans - by Yang et al. in Guangzhou, China, who
are certainly not Intactivists - in fact their experimental
group was 96 men with "redundant prepuce", i.e. normal, who were
measured before and then at monthly intervals after
circumcision.
"Extraordinary claims demand extraordinary proof," but the
Sorrells study only demonstrates what should be obvious. The
value of this study is that it is much more thorough and less
biased in its design toward circumcision than the ones below.
More studies are needed to establish the link between
touch-sensitivity and sexual pleasure, but it should be obvious
to most men.
One of the circumcised experimental subjects reports on the experience.
A presentation was given at the World Association of Sexuality
Congress in Sydney in April 2007, contrasting the Sorrells study
with Masters' & Johnson's. A
large poster accompanying the presentation can be downloaded
(pdf, 3.2MB).
A Belgian study has two potential flaws. It is
survey-based, and the measure of sexual sensitivity is by
self-report, but it has a large number of subjects
.
|
BJU Int. 2013 Feb 4. doi:
10.1111/j.1464-410X.2012.11761.x. [Epub ahead of
print]
Male circumcision decreases penile sensitivity as
measured in a large cohort.
Bronselaer GA, Schober JM, Meyer-Bahlburg HF,
T'sjoen G, Vlietinck R, Hoebeke PB.
Department of Urology, Ghent University Hospital,
Ghent, Belgium.
Abstract
WHAT'S KNOWN ON THE SUBJECT? AND WHAT DOES THE STUDY
ADD?: The sensitivity of the foreskin and its
importance in erogenous sensitivity is widely debated
and controversial. This is part of the actual public
debate on circumcision for non-medical reason. Today
some studies on the effect of circumcision on sexual
function are available. However they vary widely in
outcome. The present study shows in a large cohort of
men, based on self-assessment, that the
foreskin
has erogenous sensitivity. It is shown that the foreskin is more sensitive than
the uncircumcised glans mucosa, which means
that after circumcision genital sensitivity is lost.
In the debate on clitoral surgery the proven loss of
sensitivity has been the strongest argument to change
medical practice. In the present study there
is strong evidence on the erogenous sensitivity of
the foreskin. This knowledge hopefully can
help doctors and patients in their decision on
circumcision for non-medical reason.
OBJECTIVES:
To test the hypothesis that sensitivity of the
foreskin is a substantial part of male penile
sensitivity. To determine the effects of male
circumcision on penile sensitivity in a large sample.
SUBJECTS AND METHODS:
The study aimed at a sample size of >1000 men.
Given the intimate nature of the questions and the
intended large sample size, the authors decided to
create an online survey. Respondents were recruited by
means of leaflets and advertising.
RESULTS:
The analysis sample consisted of 1059 uncircumcised
and 310 circumcised men. For the glans penis, circumcised
men
reported decreased sexual pleasure and lower orgasm
intensity. They also stated more
effort was required to achieve orgasm, and a
higher percentage of them experienced unusual
sensations (burning, prickling, itching, or tingling
and numbness of the glans penis). For the penile shaft
a higher percentage of circumcised men described
discomfort and pain, numbness and unusual sensations.
In comparison to men circumcised before puberty, men
circumcised during adolescence or later indicated less
sexual pleasure at the glans penis, and a higher
percentage of them reported discomfort or pain and
unusual sensations at the penile shaft.
CONCLUSIONS:
This study confirms the importance of the foreskin for
penile sensitivity, overall sexual satisfaction, and
penile functioning. Furthermore, this study shows that
a higher percentage of circumcised men experience
discomfort or pain and unusual sensations as compared
with the uncircumcised population. Before circumcision
without medical indication, adult men, and parents
considering circumcision of their sons, should be
informed of the importance of the foreskin in male
sexuality.
|
Masters and Johnson
The entire basis of the claim that circumcision has no
effect on sexuality was until recently an "experiment" performed
over 40 years ago by William H. Masters MD and Virginia E.
Johnson and reported in their 1966 best-seller, "Human Sexual
Response". Their bias toward circumcision and their ignorance of
the intact penis are manifest.
|
Their first picture, of the "normal" anatomy, shows
no sign of a foreskin.
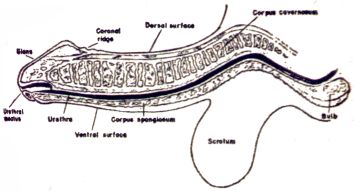
FIGURE 12-1 The penis: normal
anatomy (lateral view). (p 177)
What is labelled "coronal ridge" looks more like a
circumcision scar. The corona
(glandis) is actually the high point to the left
of that.
Their next picture shows the foreskin but does not
identify it.
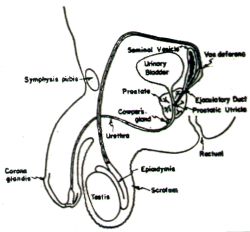
FIGURE 12-3 Male pelvis: normal
anatomy (lateral view). (p 180)
The corona glandis
is misidentified.
The next four drawings are similar to this one:
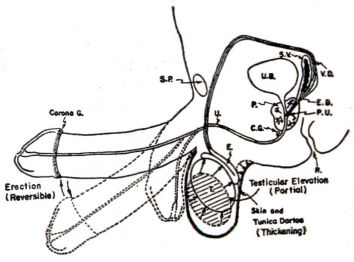
FIGURE 12-4 Male pelvis:
excitement phase. (p 182)
They look as though someone unfamiliar with the
foreskin added it to a diagram of a circumcised penis,
but it is still not identified. None of the pictures
of erections show that the foreskin can retract, or how. Thank heaven an erection
is (usually) "Reversible"!
This is actually a picture of a dissected penis (from
below) with all skin removed:
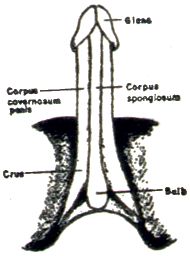
FIGURE 12-8 The penis: erect
(ventral view). (p 187)
Masters and Johnson's bias towards circumcision is
further shown by their table 2-6
|
Reproductive Organ Pathology
in Male Study Subjects
Pathology
Benign prostatic hypertophies
Unilateral testicular atrophies
Undescended testicle
Inguinal hernia (non-symptomatic)
Inguinal hernia (symptomatic)
Varicocele (symptomatic)
Additional Data
Uncircumcised
penises
|
p 17
and table 2-8
|
Surgical History of Male Study
Subjects
Major pelivic surgery
Prostatectomy
Transurethral
Perineal
Inguinal herniorrhaphy
[but not
circumcision].
|
p 18
This belies any claim to objectivity.
Their discussion of circumcision (pp 189-190) begins
with a claim that because only 16 (actually 9
according to their own table) of the 231 men aged
21-40 were intact (compared to 26 of the 81 older
men), there was "a medical trend toward urging routine
circumcision of the newborn male infant." This ignores
males under 21, and hence the most recent 21 years of
medical history. They also assume their sample of 315
volunteers (who were comfortable having sex in front
of the experimenters) was representative of the whole
population of the US, and the 35 intact ones
representative of all intact men.
They continue (in prose famous for its obscurity and
ugliness):
The phallic fallacy that the uncircumcised male can
establish ejaculatory control more effectively than
his circumcised counterpart was accepted almost
universally as biologic fact by both circumcised and
uncircumcised male study subjects. [The
popular press at the time was widely claiming
the reverse. Magazines like Penthouse
were suggesting that intact men with premature
ejaculation might get circumcised to prevent it.]
This concept was founded on the widespread
misconception that the circumcised penile glans is
more sensitive to the exteroceptive [ie, from
outside] stimuli of coition or masturbation than is
the glans protected by the residual foreskin. [A misconception indeed!
"Residual" is a prejudiced way of saying
"intact". All involved in this fallacy seem to
have been unaware that the foreskin can retract.
Masters and Johnson ignore the possiblity that
the foreskin itself is involved in sexual
sensation.] Therefore, the
circumcised male has been presumed to have more
difficulty with ejaculatory control and (as many
study subjects believed) a greater tendency towards
impotence.
A limited number of the male study-subject
population was exposed to a brief clinical
experiment designed to
disprove [Real
scientists aim to test, not prove or disprove]
the false
premise [If it had not yet
been disproved, how did they know it was false?]
of excessive sensitivity of the circumcised glans.
The 35 uncircumcised males were matched at random
with circumcised study subjects of similar ages. Routine neurologic testing for
both exteroceptive and light tactile
discrimination were conducted on the ventral and
dorsal surfaces of the penile body, with
particular attention directed toward the glans.
[No further details are
given as to the nature of these tests and it
has proved impossible to find out. It is
unclear what "particular attention" means. It
goes without saying that no attention was given
to the foreskin, nor could it be with the
circumcised "male study subjects".]
No clinically significant difference could be
established between the circumcised and the
uncircumcised glans
during these examinations. [Surprise!
Masters
and Johnson didn't find what they weren't
looking for. NB: this testing was purely for the
sense of touch. It had nothing to do with sex.]
An elaborate explanation of this "finding" follows,
based on Masters and Johnson's observation that 29 out
of the 35 "uncircumcised male study subjects" had
foreskins that retracted during intercourse. They were
apparently previously unaware that foreskins usually
retract.
This is linked to a later (p197) discussion of
"automanipulation" (masturbation):
Uncircumcised males have not been observed to
concentrate specifically on the glans area of the
penis. [Of course not!
They were playing with their much more sensitive
foreskins but Masters and Johnson failed
to notice that.] Normally they follow
the usual pattern of confining manipulative activity
entirely to the penile shaft [of
which
the foreskin is an integral part].
Stroking techniques rarely move sufficiently distal
on the shaft of the penis to encounter more than the
coronal ridge of the glans even late in plateau
phase just before ejaculation. [The
coronal
ridge is quite sufficient, forming an anvil on
which to rub the foreskin.]
Masters and Johnson conspicuously fail to notice a
common technique of intact men, of using only one or
two fingers and the thumb to move the foreskin on and
off the glans - which contrasts sharply with the
furious grasping, squeezing and grinding of the shaft
and glans by circumcised men.
Masters and Johnson's only interest in the foreskin
in intercourse is whether it covers the glans:
This is obviously a different picture from that
occasioned by active intercourse. With full vaginal
containment the foreskin not tightly attached to
subjacent tissue usually retracts freely from a
major portion of the glans during active male coital
thrusting before ejaculation.
|
On this was based the whole of the case that "circumcision has
no effect on sexual function" until further studies with flaws
of their own (see below) were used to make the same claim.
In "Dear Dr HIPPocrates", Dr Eugene Schoenfeld elaborates it to
"As for the question of decreased sensitivity of the glans,
Masters and Johnson studied this question in their researches
into the physiology of sex. Extensive
neurological testing of such sensations as touch and pain
sensitivity failed to reveal any differences in those with and
without foreskins."
In "Healthy Sex" by Miriam Stoppard (Dorling Kindersley), the
claim about a myth of greater control by intact men, and the
alleged reason for it, is paraphrased almost verbatim, without
acknowledgement.
The claim of "no effect" was quoted as recently as February
2002 in the American Association of
Family Physicians' Policy Statement.
|
"What were those experiments?"
In January 2001, PhD student Tina Kimmel tried to
find out just what the experiments were that have
proved so influential in maintaining the claim that
"circumcision has no effect on sexuality".
William H. Masters, 85, was in a nursing home in
Arizona with Parkinson's disease and had no memory of
the experiments. He died a few weeks later.
Collaborator Robert Kolodny said that he never once
heard Masters or Johnson refer to this study, but
thought Masters might have done it in collaboration
with his physiologist at the time, Dr. William Slater.
Slater died years ago.
Kolodny says most of the research notes from that
period have been discarded, because of the rising
costs of storage.
He guessed that "light tactile discrimination" meant
single-point threshold sensitivity, although he had no
idea what "exteroceptive discrimination" meant.
Ms Kimmel could not reach Virginia Johnson in St.
Louis, but everyone she spoke to thought Johnson was
most probably not involved in the study at all.
|
(It has recently been suggested that Masters
and
Johnson faked the evidence for their claim of converting
78% of willing subjects from homosexuality to heterosexuality.)
|
In sharp contrast is the
importance Masters and Johnson attach to the role of
the clitoral hood (female prepuce) in intercourse:
A mechanical traction
develops on both sides of the clitoral hood of the
minor labia subsequent to penile distention of the
vaginal outlet. With active penile thrusting, the
clitoral body is pulled downward toward the
pudendum [Masters and
Johnson define the "pudendum" as "the mons
pubis, labia majora, labia minora, and the
vestibule of the vagina".] by
traction exerted on the wings of the clitoral
hood....
When the penile shaft is in
the withdrawal phase of active coital stroking,
traction on the clitoral hood is somewhat relieved
and the body and glans return to normal
pudendal-overhang positioning....
... If the vaginal outlet is
too expanded to allow strong traction on the
minor-labial hood by the thrusting penis, minimal
clitoral excursion will occur and little if any
secondary stimulation will develop.
- p.58
But the role they attach to the
female prepuce is still a passive one, and they do
not consider the possibility that it may be the
source of erotic sensation in its own right, either.
In "The Hite Report"
(Dell/Summit, 1977, p. 271) and "The New Hite
Report", Shere Hite grants the importance of the
role of the clitoral hood, but pours scorn on
Masters and Johnson's emphasis on the role of
"active penile thrusting" calling it "a Rube
Goldberg model".
In response to an enquiry about the role of the
clitoral hood, "Charlou" at RichardDawkins.net
wrote:
|
Direct
stimulation of my clitoris concentrates
the sensation too intensely for me,
particularly close to and during clitoral
orgasm. Manipulation over and around the
hood and labia is both exquisitely
pleasurable and extends the orgasm. Often
controlling and delaying the clitoral
orgasm this way generates a deeper
internal orgasm. Oooohlalallaaaaaaaa...
|
|
A more recent study makes the same mistake, perhaps more
glaringly. Abstract
of a paper presented at a meeting of the American Urological
Association in Chicago on April 29, 2003.
| Publishing ID:
1260 |
Abstract ID:
100769 |
EFFECTS OF CIRCUMCISION ON MALE
PENILE
SENSITIVITY
Clifford B Bleustein*, Haftan
Eckholdt, Joseph C Arezzo, Arnold Melman, Bronx, NY
Introduction and Objective: Controversy
continues to exist about the effect of circumcision on
penile sensitivity and sexual satisfaction. This study
was designed to evaluate penile sensitivity in both
circumcised and uncircumcised males. We evaluated both
large and small axon nerve fibers using vibration,
pressure, spatial perception, and warm and cold
thermal thresholds. Measurements both in functional
men and men with erectile dysfunction (ED) were
obtained to evaluate for differences in penile
sensitivities.
Methods: Seventy-nine patients were evaluated.
In the cohort evaluated, 54% (43/79) were
uncircumcised, while 46% (36/79) were circumcised. All
patients completed the erectile function domain of the
International Index of Erectile Function (IIEF)
questionnaire. Patients were subsequently tested on the dorsal midline glans of the
penis. In uncircumcised males, the foreskin was
retracted for testing. [They
compared the exterior of the foreskin with
the glans, while it is the interior where the ridged band
is] Vibration (Biothesiometer),
pressure (Semmes-Weinstein monofilaments), spatial
perception (Tactile Circumferential Discriminator),
and warm and cold thermal thresholds (Physitemp NTE-2)
were measured. [These tests
are all tuned to the kinds of sensitivity the
glans is best at.] Bivariate
relationships were assessed using chi square, t test,
and Pearson correlations. [With
such small samples, such sophisticated statistical
methods are suspect.] Composite null
hypotheses were assessed with mixed models repeated
measures analysis of variance allowing us to covary
for age, diabetes, and hypertension.
Results: Functional group t test analysis only
demonstrated a significant (p= 0.048) difference for
warm thermal thresholds with a higher threshold (worse
sensation) for uncircumcised men. However,
significance was lost when we controlled for age,
hypertension, and diabetes. For the dysfunctional
groups t test analysis only demonstrated a significant
(p= 0.01) difference for vibration (biothesiometry)
with a higher threshold (worse sensation) for
uncircumcised men. Again, this also lost significance
(p=0.08) when controlling for age, hypertension, and
diabetes. We also found that overall race is related
to circumcision status with Caucasian men 25 times and
African American men 8 times more likely to be
circumcised than Hispanics.
[Again, with such a small
and non-random sample - all urology patients - it
is preposterous to generalise to the whole
population. This breaks down to actual numbers as
30 out of 34 white men
(88%)
5 out of 17 black men (29%) and
1 out of 28 Hispanic men (3.6%) having been
circumcised.
An enormous amount hangs on
that one circumcised Hispanic man: if just one other
was circumcised, Melman et al.'s figures would fall
to 12.5 times and 4 times as likely - and if he had
been left intact, they would have found Caucasians
and Blacks are infinitely more likely to
circumcise than Hispanics! This is irrelevant to
sensitivity, but its innumeracy casts grave doubt on
the rest of the research. ]
Conclusions: We present a comparative analysis
between uncircumcised and circumcised men using a
battery of quantitative somatosensory tests that
evaluate the spectrum of small to large axon nerve
fibers. We demonstrated that there are no significant
differences in penile [glans]
sensation between [these]
circumcised and uncircumcised men with respect to
vibration, spatial perception, pressure, warm and cold
thermal thresholds in both patients with and without
erectile dysfunction.
|
Bossio et al. measured only the
outside of the foreskin, and ignored their finding that it was
more sensitive to touch
|
Journal of Urology
Examining Penile Sensitivity in Neonatally
Circumcised and Intact Men Using Quantitative Sensory
Testing
Jennifer A. Bossio, Caroline F. Pukall, Stephen S.
Steele
DOI: http://dx.doi.org/10.1016/j.juro.2015.12.080
Abstract
Purpose
Little is known about the long-term implications of
neonatal circumcision on the penile sensitivity of
adult men, despite recent public policy endorsing the
procedure in the United States. [It
did not.] In the current study we
assessed penile sensitivity in adult men by comparing
peripheral nerve function of the penis across
circumcision status.
Materials and Methods
A total of 62 men (age 18 to 37 years, mean 24.1, SD
5.1) completed study procedures (30 circumcised, 32
intact). [That's very few from
which to generalise. Men with sexual dysfunction
were excluded by design.] Quantitative
sensory testing protocols were used to assess touch
and pain thresholds (modified von Frey filaments) and
warmth detection and heat pain
thresholds (a thermal analyzer) [What
does
heat pain have to do with sexual
pleasure?] at a control site (forearm)
and 3 to 4 penile sites (glans penis, midline shaft,
proximal to midline shaft
[It is not clear why two
so similar sites on the shaft were chosen,
rather than more
divergent sites, such as the 19 used by
Sorrells et. al, including the frenulum,
the ridged band and the circumcision scar.]
and foreskin, if present
[and of course when it is not
present it has no sensitivity at all] ).
[Here is where they measured
the sensitivity of the foreskin:
It would be surprising if
this tested any differently from the rest of the
shaft.]
Results
Penile sensitivity [at
those three points on the cut penis]
did not differ across circumcision status for any
stimulus type or penile site. The
foreskin of intact men was more sensitive to
tactile stimulation than the other penile sites,
but this finding did not extend to any other stimuli
(where foreskin sensitivity was comparable to the
other sites tested). [The
foreskin of cut men was completely
insensitive, having been cut off and thrown away
18-37 years ago. This self-evident observation is
the elephant in the room.]
[The full text says: "Similar to Sorrells et
al.[9], we found that—of
all the genital sites tested—the foreskin was
the most sensitive to tactile sensation stimuli.
However, given the high prevalence of fine-touch
pressure receptors (Meissner corpuscles) in the
preputial mucosa, this finding was not
unexpected." They somehow think that because it is
not unexpected, it can be ignored, because they
proceed to ignore it.
They express the result in this graphic
(colouring and emphasis mine):
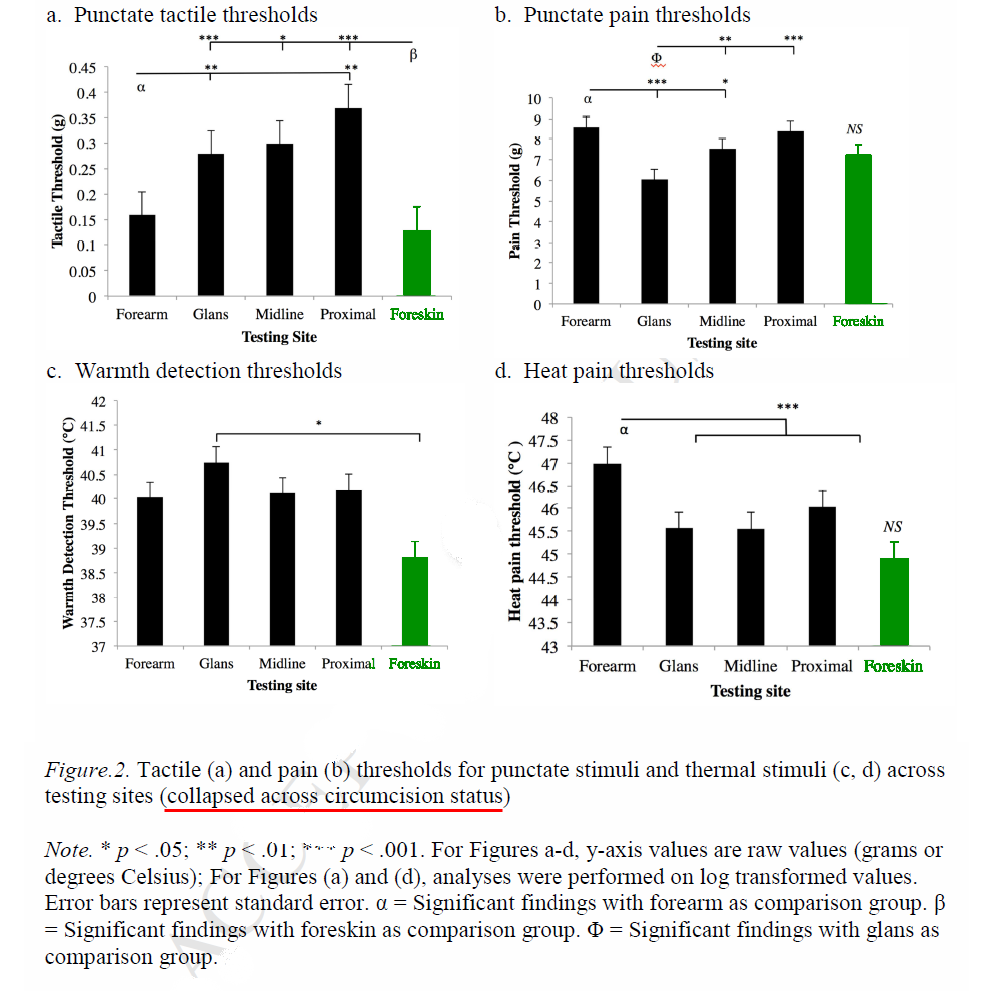
It glosses over the fact
that the cut men have no foreskin sensitivity
whatsoever.]
Conclusions
Findings suggest that minimal long-term implications
for penile sensitivity exist as a result of the
surgical excision of the foreskin during neonatal
circumcision [If you ignore
the fact that you are significantly reducing the
total innervation of the penis.]
Additionally, this study challenges past research
suggesting that the foreskin is the most sensitive
part of the adult penis. [?]
Future research should consider the direct link
between penile sensitivity and the perception of
pleasure/sensation. Results are relevant to policy
makers, parents of male children [but
not to adult men?] and the general
public.
Key Words:
circumcision, male, infant, newborn, penis, sensation,
sensory thresholds [but
not prepuce or foreskin] |
And again:
|
J Sex Med. 2007 Apr 6; [Epub ahead of print]
Sensation and Sexual Arousal in Circumcised and
Uncircumcised Men.
Payne K, Thaler L, Kukkonen T, Carrier S, Binik Y.
Riverside Professional Center, Ottawa, Canada
Introduction. Research, theory, and popular
belief all suggest that penile sensation is greater in
the uncircumcised as compared with the circumcised
man. However, research involving direct measurement of
penile sensation has been undertaken only in sexually
functional and dysfunctional groups, and as a
correlate of sexual behavior. There are no reports of
penile sensation in sexually aroused subjects, and it
is not known how arousal affects sensation. In
principle, this should be more closely related to
actual sexual function.
Aim. This study therefore compared genital and
nongenital sensation as a function of sexual arousal
in circumcised and uncircumcised men.
Methods. Twenty uncircumcised men and an equal
number of age-matched circumcised participants
underwent genital and nongenital sensory testing at
baseline and in response to erotic and control
stimulus films. Touch and pain thresholds were
assessed on the penile shaft, the glans penis, [but not the foreskin]
and the volar surface of the forearm.
[volar = of the palm - meaning upper when the palm is
up?] Sexual arousal was assessed via thermal imaging [of one small region]
of the penis.
Results. In response to the erotic stimulus,
both groups evidenced a significant increase in penile
temperature, which correlated highly with subjective
reports of sexual arousal. Uncircumcised men had
significantly lower penile temperature than
circumcised men, and evidenced a larger increase in
penile temperature with sexual arousal.
[This is news, suggesting
the foreskin functions as a radiator - but the
surface of the one small region of the penis they
measured, "just below {proximal
to?} the glans penis, adjacent to the coronal
ridge on the lateral right surface of the penile
shaft" is skin on the intact man, but may be
mucosa on the circumcised. Since they ignore the
foreskin, they also ignore the fact that the
foreskin rolls back on arousal, so that mucosa is
exposed on both.]
No differences in genital sensitivity were found
between the uncircumcised and circumcised groups.
Uncircumcised men were less sensitive to touch on the
forearm than circumcised men [Suggesting
overall hypersensitivity is a long-term
consequence of circumcision?]. A
decrease in overall touch sensitivity was observed in
both groups with exposure to the erotic film as
compared with either baseline or control stimulus film
conditions. No significant effect was found for pain
sensitivity.
Conclusion. These results do not support the
hypothesized penile sensory differences associated
with circumcision [so long
as you ignore the foreskin]. However,
group differences in penile temperature and sexual
response were found.
PMID: 17419812 [PubMed - as supplied by publisher]
In the full text, it says :
Discussion
... It is possible that the uncircumcised penis is
more sensitive due to the presence of additional
sensory receptors on the prepuce and frenulum, [Possible? It should be
blindingly obvious. The receptors a baby is born
with are not "additional"] but this
cannot be compared with the absence of such
structures on the circumcised penis. [Something
cannot be compared with nothing, but that
doesn't mean something doesn't exist or is
irrelevant. They could have compared the
senstivitities of the prepuce and intact
frenulum with those of the glans and shaft.]
This notwithstanding, the present data do cast doubt
on the notion that the glans penis is more sensitive
in the uncircumcised man due to the protective
function of the prepuce. [Doubt
perhaps,
but this begs the question that glans
sensitivity is all that matters. Note also that
this perfectly reasonable supposition is demoted
to a "notion".] Possible explanations
for the origin of such a belief may date back to
historical traditions, whereby circumcision was
performed in order to reduce sexual gratification
[22], or to prevent masturbation [23]. This may have
led to the general notion that circumcised men were
somehow "less sexual" and therefore less "sexually
sensitive" than uncircumcised men. [Got
that? "People got the false idea that
circumcision reduces sensitivity because they
circumcised with that purpose." Or could they
possibly have done it because it does? These
pages consider other effects
of glans exposure.]
Conclusion
... In light of these findings, the examination of
penile sensory diffrences between uncircumcised and
circumcised men warrants further study via a
replication with a larger sample size [Sorrells et al. had
this] including the measurement of
multiple sensory modalities over multiple penile
locations (comprising those believed to be directly
affected by circumcision [i.e.
the foreskin, and Sorrells et al. did this])....
22 Maimünides [sic] M. The
guide for the perplexed. Shlomo P, tr.
Chicago, IL: University of Chicago Press; 1963.
23 Moscucci O. Clitoridectomy, circumcision, and the
politics of sexual pleasure. In: Miller AH, Adams
JE, eds. Sexualities in Victorian Britain.
Bloomington, IN: Indiana University Press;
1996:60-78.
[Conspicious by their
absence from these citations are Sorrells
et al. and
Taylor et al.]
|
The authors of this study tried as hard as they could to
ignore the effect of circumcision
|
BJU International 103 (2009), 1096 – 1103
Self-ratings of genital anatomy, sexual sensitivity
and function in men using the 'Self-Assessment of
Genital Anatomy and Sexual Function, Male'
questionnaire
Justine M. Schober, Heino F.L. Meyer-Bahlburg and
Curtis Dolezal
[This study will be hard for
European and other intact men to comprehend,
without adopting the authors' apparent assumption
that circumcision is not genital surgery
and has no effect on the parameters measured.]
|
OBJECTIVE
To assess the perceptions of healthy men of
their genital anatomy and sexual sensitivity,
along with the re-test reliability of these
ratings, in a new self-reported questionnaire,
the Self-Assessment of Genital Anatomy and
Sexual Function, Male (SAGASF-M).
SUBJECTS AND METHODS
Eighty-one healthy, sexually active, men aged
22–57 years (median 33), with no
history
of genital surgery, completed the
SAGASF-M.
...
RESULTS
...Ranked by degree of 'sexual pleasure', the
area 'underside of the glans' was highest,
followed by 'underside of the penile shaft',
'upper side of the glans', 'left and right
sides of the glans', 'one or both sides of the
penis', 'upper side of the penile shaft', 'foreskin' (11 subjects),
'skin between the scrotum and anus', 'back
side of the scrotum', 'front side of the
scrotum', and 'around anus', but not all pair
differences were significant.
CONCLUSION
The SAGASF-M discriminates reasonably well
between various genital and nongenital areas
in terms of erotic sensitivity, when
administered to genitally
unoperated men varying widely in age
and socio-economic level.
|
...
SUBJECTS AND METHODS
For this methodological study we targeted
English-speaking men with no
history of genital surgery and with a
variable educational background.
...
Given that this was a largely healthy sample with
no history of genital surgery, the initial
ratings of genital anatomy, which showed little
variability, are not described here. [It
might
have been interesting, with sufficient sample
size, to compare intact and circumcised men's
rating of their genital anatomy.]
...
Note that, because there were few (11) uncircumcised
men in this sample, 'area A/foreskin' was excluded
from statistical analysis, but for comparison purposes
included in the Fig. 2B–E). Ranked by degree of
'sexual pleasure' (Table 1), the area 'underside of
the glans' [Yes, the
frenulum, in circumcised men the last remnant of
Taylor's ridged
band] was highest, followed by
'underside of the penile shaft', 'upper side of the
glans', 'left and right sides of the glans', 'one or
both sides of the penis', 'upper side of the penile
shaft' '(foreskin)' [apparently
they
merged foreskin measurements with upper shaft
measurements for no apparent reason],
'skin between the scrotum and anus', 'back side of the
scrotum', 'front side of the scrotum', and 'around
anus', but not all pair differences were significant.
...
Surgical modification or removal of genital tissue,
as it occurs in genital reconstruction surgery or circumcision, increases the potential [just the
potential?] for (objective) variations in sensory
thresholds and might
also alter structural integrity, meatal
position, straightness during erection, erectile
capacity, and personal and partner views of cosmesis
[25–27]. In recent years, genital surgery, especially
when done without the patient's consent as is common
in intersex children [and
very common in normal boys], has come
under harsh criticism by patients, because of
recurrent reports of the experience after surgery of
poor cosmetic quality and/or impaired sexual
functioning in adulthood [28]. Some intersex activists
have even called for a moratorium on genital surgery,
until more adequate followup data are provided [29]. ["Even"? Is that so outlandish,
just to be left alone?]
...
Men with a history of genital masculinizing surgery
or genital excision surgery were excluded.
Circumcision status was documented, but this genital
surgery was not an exclusion criterion.
[The only time they admit
that circumcision is genital surgery. If it had
been an exclusion criterion, they would only have
had 11 subjects! Intact and circumcised subjects
should certainly have been treated separately on
all measures.]
DISCUSSION
... The present study provided somewhat surprising
data on orgasmic sensitivity. Both the ventral penile
shaft and the area of the ventral glans penis were
rated at an almost equal level of orgasmic sensitivity
and sexual pleasure, significantly above the levels of
all other areas rated. This is different from what
might be expected, considering the nerve density shown
by Yucel and Baskin's example of the fetal penis. The
terminal nerves there end in the
foreskin and dorsal glans. The difference
noted in the present study might be a consequence of
the high circumcision rate of the respondents of the
study. When terminal nerves are
excised, a dermatome [area of skin served by one
spinal nerve] might migrate. It could also be
that sexual sensitivity ratings include a
pressure-related sensation rather than only a
fine-touch or tactile sensation.
[Now what we need is someone
to use the SAGASF-M with more sagasfity, comparing
and contrasting intact men with circumcised.]
|
Removal of the foreskin does affect the surface of the glans.
It becomes keratanised,
covered in a hardened coating. This shields the nerves of the
glans from stimulation.
These two effects together combine to change the quality, and
reduce the quantity, of sensitivity of circumcised men. The
neurology has not been studied in detail, but other work
suggests that when nerves are severed in infancy they
reconfigure themselves -
|
Fetal and infant brains exhibit an admirable
adaptability to unique developmental
conditions—whether those conditions are unique to
individuals within a species (as with armless wonders
[people born without arms]) or are unique among
species (as with jerboas [long-legged jumping rats]).
This adaptability is essential given the unpredictable
size and conformation of our bodies. Predetermined
brain function is neither feasible nor desired.
Instead ...
the functional organization of the nervous system
reflects how it interacts during development with its
particular sensory and motor systems.
That individuals can exhibit compensatory responses
to sensory loss might be familiar even to people who
have not met an "armless wonder." Have you ever
wondered whether the extraordinary musical ability of
Stevie Wonder owes anything to sensory compensation
resulting from his congenital blindness? There is now
evidence that it does. Moreover, sensory compensation
is accompanied by brain reorganization. For example,
in congenially blind humans, the part of the cerebral
cortex that, in sighted people, would process light
arriving from the eyes is recruited to process tactile
information arriving from the fingers. This
reorganization was demonstrated experimentally by
disrupting the functioning of the "visual" part of the
brain (by exposing it to powerful magnetic
stimulation) as blind individuals used their fingers
for Braille reading. This stimulation distorted the
tactile perceptions of these blind subjects, whereas
similar manipulations of the brains of sighted
individuals disrupted vision without affecting
tactile perceptions. Thus, even after millions of
years of processing visual information, the mammalian
"visual" cortex remains open to inputs from other
sensory systems.
This reorganization of the cerebral cortex also has
been observed in short-tailed opossums that were
experimentally blinded soon after birth. When their
adult brains were examined, sensory maps of the brain
surface showed extensive encroachment of the areas
responding to sound and touch into areas that, in a
sighted animal, would respond only to light. We
might say that in the absence of visual stimulation, the visual cortex is colonized by other
sensory systems.
... For all of the reasons discussed so far, it is
clear that sensory organs on
the periphery "instruct" the developing brain to
produce functional map-like representations.
But this instruction is not mindless. On the contrary,
it appears that the final organization of the cortex
reflects the structure of the peripheral organ and
the uses put to that organ early in development. ...
We know from research in human adults that experience
sach as playing a stringed instrument—can modify
cortical organization. Such experience is even more
profound in early infancy, when the most fundamental
relationships between peripheral structures and the
brain—and among systems within the brain—are being
established. When new sensory structures arise ...
they take advantage of the inherent plasticity of the
infant brain to make sense of the sensory information
provided. One neuro-scientist sums up these
relationships in one simple sentence: "The developing
nervous system is also an evolving nervous system."
Every undergraduate, graduate, and medical student
learning about the brain must memorize the various
lobes of the cerebral cortex and their particular
roles in vision, hearing, touch, and smell. I
certainly did. But such lessons in memorization are
rarely accompanied by the caveat that our current
discussion demands: that each lobe of the brain
reliably can be ascribed a particular function only
because the eyes, ears, fingers, and nose reliably
send their neural connections to particular locales
within the brain.
Thus, our brains are not preprogrammed to expect
the presence of any appendage, whether arms, legs
[or] eyes .... Rather, it is the reliability of
sensory targeting (and other developmental factors)
that produces the illusion of a preprogrammed
brain. So, if we were to examine the brain of an
armless wonder, we would find a cerebral cortex that
lacks map-like representations of the missing arms. In
their place, we would discover enlarged
representations of legs, feet, and toes. [And
if we were to examine the brain of a circumcised
man, we would find a cerebral cortex that lacks a
map-like prepresentation of the missing foreskin.
In its place, we would discover an enlarged
representation of the glans and frenulum.]
- "Freaks of Nature" by Mark S.
Blumberg,
Oxford (2009) pp 146-7, 150-1
|
- so that men circumcised in infancy find pleasure in
stimulation of the glans (for which it was not designed / did
not evolve) that intact men do not. This suggests that men
circumcised in adulthood react differently from men circumcised
as babies:
|
All of us must learn how our particular bodies work.
We are not hardwired for sex and there is no innate
instruction manual. Getting sex right, for our
partners and us, entails many trials and a lot of
errors. As with any learning process, feedback is
essential. Slicing away at sexual organs to produce a
cosmetic improvement severs communication between
genitals and brain, thereby thwarting the very
learning process that makes the development of sexual
behavior possible.
ibid p211 (in the context of gender
assignment surgery)
|
- When a man is circumcised in adulthood, his loss of
sensation has been well documented elsewhere.
It has been compared to sight without colour, hearing with one
ear or seeing with one eye.
|
Errol Morris, the filmmaker, was born with strabismus and subsequently
lost almost all the vision in one eye, but feels
he gets along perfectly well. "I see things in
3-D," he said. "I move my head when I need to - parallax is enough. I don't
see the world as a plane." He joked that he
considered stereopsis [3D vision] no more than a
"gimmick" and found my interest in it "bizarre."
I tried to argue with him, to expatiate on the special
character and beauty of stereopsis. But one cannot
convey to the stereo-blind what stereopsis is
like; the subjective quality, the quale, of stereopsis is
unique and no less remarkable than that of color.
However brilliantly a person with monocular vision
may function, he or she is, in this one sense,
totally lacking.
...
With prismatic spectacles and exercises, Sue
Barry recovered stereo vision after a lifetime
of using her two eyes separately:
I went back to my car and happened to glance at
the steering wheel. It had "popped out" from the
dashboard. I closed one eye, then the other,
then looked with both eyes again, and the
steering wheel looked different. I decided that
the light from the setting sun was playing
tricks on me and drove home. But the next day I
got up, did the eye exercises., and got into the
car to drive to work. When I looked at-the
rear-view mirror, it had popped out from the
windshield.
Her new vision was "absolutely delightful," Sue
wrote. "I had no idea what I
had been missing."
- Oliver Sacks, The Mind's Eye
|
It includes both the immediate loss of sensation from the
foreskin itself, and the progressive desensitisation of the
glans as the surface keratinises.
Immediately after circumcision, the nerves of the glans
bombard the brain with the new sense impressions they are
constantly receiving, which the brain interprets as pain.
(Newly circumcised men are advised to wear loose clothing -
none if this is practicable.) This fades over time. One
reason will be that the brain learns to disregard these
signals, like any other constant sensation. They have been
called "false alarms".
- In the case of infant circumcision, the position is rather
more complicated. The boy develops his sexuality with what he
has left. We may speculate that the portion of the sensory
region of the brain that was expecting signals from the
foreskin is colonised by nerves from adjacent areas, such as
the glans, with the result that the glans of an
infant-circumcised man becomes erogenous in a way that the
glans of an intact man does not. There is anecdotal evidence
for this.
That explains why infant-circumcised (but not
adult-circumcised) men commonly say
"I couldn't cope with any more sensitivity than I have
now."
or
"If I was any more sensitive I'd have a heart attack!"
The sensitivity they have left, from their glanses, and which
intact men do not experience as pleasure, is closely allied to pain.
The quality of sensation from the foreskin is quite different,
more like tickling. This would also suggest that circumcised men
have a more hair-trigger kind of sensitivity. Having fewer
nerves available to stimulate the centres that lead to
ejaculation and orgasm, the nerves they have must work harder.
Thus it could well be true that "the circumcised male has more
difficulty with ejaculatory control."
Circumcision changes not only the amount but the kind
of sensitivity
of the glans, as well as removing all the sensitivity of
the foreskin, except the anomalous stimulation from cut-off
nerves that have formed the growths known as neuromas.
|
Marilyn Milos writes:
I
have dealt, time and again, with talk show hosts who
say "If I had any more sensitivity, I couldn't stand
it." I think the reason for this is that, without
the Meissner's
corpuscles in the ridged
band of the foreskin to provide sensory
feedback, a man doesn't know where he is in relation
to the orgasmic threshold. Many men think their
inability to control orgasmic timing is due to
over-sensitivity rather than the fact the lack tens
of thousands of important nerve endings that provide
essential feedback.
|
In fact, men who
talk like those hosts implicitly condemn circumcision for
making their sensitivity too hair-trigger. (This growing
collection of anecdotes is on another page.)
This also suggests a mechanism for what has often been noted
informally (and complained of by women), that circumcised men
are more goal-oriented about sex. Getting to orgasm is more
important than any pleasures to be had on the way. Circumcised
men commonly say that there is nothing wrong with their
sexuality because "I
can still reach ejaculation and orgasm". (This growing
collection of anecdotes is on another page.)
When the ridged band is missing, the nervous connection between
stimulation and arousal is so thin (the "bandwidth" is so low,
if you like), that the level of stimulation has to be high and
uninterrupted to reach orgasm at all. Thus circumcised men can
only relax and enjoy sex when orgasm has been reached, and
orgasm is something that has to be achieved, it may not be
pleasurably delayed. (A sex manual of 1961, "The Marriage Art"
by John D. Eichenlaub, nowhere mentions the foreskin, but
recommends that a woman apply ice to her partner's perineum
for a special thrill.)
Circumcised men commonly find their frenulum
(that is, whatever remnant of their ridged
band was left on them) to be the most sensitive part of
their penis. Many sex manuals assume this is true for all men.
None has questioned why sexual sensitivity should be so
concentrated.
|
The Laumann study
Like Masters and Johnson, the
Laumann study "Circumcision
in the United States: prevalence, prophylactic
effects, and sexual practice" is widely
misrepresented as "showing that circumcised men enjoy
more varied sexual practices and less sexual
dysfunction than intact men."
It was extracted from a much larger study that was
not designed to study circumcision. It relied on
self-reporting to determine circumcision status.
Self-reporting has been shown to be remarkably
inaccurate in other studies.
In statements that have been much
more
widely broadcast than the original study, Edward
Laumann himself misquoted his own study:
"We were quite surprised to see such clear
evidence, at least within the white population, that
masturbation was correlated with being circumcised
as well as engaging in oral sex and anal sex."
The reference to the white population is usually left
out. The reference to anal sex is false. This CNN
report later says
"Circumcised men were found to be nearly 1.4 times
more likely [as likely]
to engage in heterosexual oral sex than
uncircumcised men, the study reported. They also
were more likely to have had homosexual oral sex and
heterosexual anal intercourse."
The only significant results of the study are:
Masturbation
Of white men (N=1067, to p<=0.05 t test), 50% of
circumcised men said they had masturbated as much as
once a month or more in the last year, vs 34% of
intact men. (That figure sounds suspiciously low.)
Heterosexual oral sex
Again, only white men (84% of circumcised vs 73% of
intact) said they had ever experienced either
"active" or "passive heterosexual oral sex" and black
men (N=189, 71% of circumcised vs 57% of intact) had
ever had "passive heterosexual oral sex" only - but
these terms are not defined.
Homosexual oral sex
Only Hispanics (N=90) and only "active" (10% of
circumcised vs 2% of intact)
Heterosexual anal sex
NOT AT ALL. In no group was there a significant
difference.
Notice that the actual differences are quite small,
or in the case of homosexual oral sex, the actual
prevalence is small. They are quoted as if ALL
circumcised men have much more of ALL the practices
than ANY intact man.
To draw any conclusions from these results, whether
"circumcision makes men enjoy sex more" or
"circumcised men desparately seek out more varied
practices to make up for what they have lost", is
beside the point when the data are so weak.
Such significance as there is can readily be
explained by class-differences and more conservative
attitudes towards sex in general of classes that are
less likely to circumcise.
Sexual dysfunction
CNN: "The study found circumcised men have a slightly
lower risk of sexual dysfunction, especially later in
life."
WRONG: The study found circumcised men over 44 are
somewhat less likely to report certain kinds of sexual
dysfunction, but not others, than intact men over 44 -
but that kind of result doesn't make headlines.
The study asked the men if they had ever experienced
"lack of interest in sex, unable to ejaculate,
ejaculated prematurely, experienced pain during sex,
did not enjoy sex, was anxious about performance, had
trouble achieving/maintaining erection". (Some of
those categories overlap: a man who experienced pain
during sex would probably not enjoy sex, for example.)
Only in men aged 45-59 (N=340) were there any
significant differences:
- 37% of the intact men reported premature
ejaculation, vs 25% of the circumcised men
- 22% of the intact men reported performance
anxiety, vs 13% of the circumcised men
- 29% of the intact men reported trouble achieving
or maintaining erection vs 13% of the circumcised
men. Only this measure achieved significance for men
of all ages (17% of all the intact men vs 10% of all
the circumcised men).
The measure "had any dysfunction" - apparently a
summation of the others - was significant only for the
45-59 age group (58% of the intact men vs 40% of the
circumcised men).
It needs some explaining why cutting part of the
penis off could make it easier to achieve or maintain
an erection, but no explanation is forthcoming.
For the actual study, see http://www.cirp.org/library/general/laumann/
|
Men cut as adults:
| Zhonghua
Nan Ke Xue. 2004 Jan;10(1):18-9.
Erectile function evaluation after
adult circumcision
[Article
in Chinese]
Shen
Z, Chen S, Zhu C, Wan Q, Chen Z.
Department of Urology, First Affiliated Hospital,
School of Medicine, Zhejiang University, Hangzhou,
Zhejiang 310003, China. shenzhj@mail.hz.zj.cn
OBJECTIVE:
To evaluate the erectile function of adults after
circumcision.
METHODS: Ninty-five patients were investigated on
erectile function by questionnaire before and after
circumcision, respectively.
RESULTS: Eighteen patients suffered from mild
erectile dysfunction before circumcision, and 28
suffered from mild or moderate erectile dysfunction
after circumcision(P = 0.001). Adult circumcision
appeared to have resulted in weakened erectile
confidence in 33 cases (P = 0.04), difficult
insertion in 41 cases (P =0.03), prolonged
intercourse in 31 cases (P = 0.04) and improved
satisfaction in 34 cases (P = 0.04).
CONCLUSIONS: Adult
circumcision has certain effect on erectile
function, to which more importance should be
attached.
PMID:
14979200 [PubMed - in process]
[This is quite a small sample,
and it is not clear why the men were
circumcised, but what makes it interesting is
that the social climate in China, unlike the US,
would not predispose them to circumcision, nor
very much against it.]
|
Absence of evidence is not evidence of absence.
|
BJU
International
January 2008
The effect of male circumcision on sexual
satisfaction and function, results from a randomized
trial of male circumcision for human immunodeficiency
virus prevention, Rakai, Uganda
Godfrey Kigozi, Stephen Watya, Chelsea B. Polis,
Denis Buwembo, Valerian Kiggundu, Maria J. Wawer,
David Serwadda, Fred Nalugoda, Noah Kiwanuka, Melanie
C. Bacon, Victor Ssempijja, Frederick Makumbi and
Ronald H. Gray
OBJECTIVE
To investigate the relationship between adult male
circumcision and sexual satisfaction and function in
men, as observational studies on the effect of adult
male circumcision on sexual satisfaction show
conflicting results.
SUBJECTS AND METHODS
We investigated self-reported sexual satisfaction and
function among men enrolled in a randomized trial of
male circumcision for human immunodeficiency virus
(HIV) prevention conducted in Rakai, Uganda. In all,
4456 sexually experienced HIV-negative males aged
15–49 years were enrolled; 2210 were randomized to
receive immediate circumcision (intervention arm) and
2246 to circumcision delayed for 24 months (control
arm). Men were followed up at 6, 12 and 24 months, and
information on sexual desire, satisfaction and
erectile dysfunction was collected. These variables
were compared between the study arms and over time
within the study arms, using chi-square or Fisher's
exact tests. The trial registration number is
NCT00425984.
RESULTS
There were no differences between the study arms at
enrolment and problems with sexual satisfaction and
function were reported by <2% of participants in
both study arms at all time points. At 6 months, no
difficulty with penetration was reported by 98.6% of
circumcised men and 99.4% of controls (P = 0.02), and
no pain on intercourse was reported by 99.4%
circumcised and 98.8% of uncircumcised men (P = 0.05).
There were no differences between the study arms in
penetration or dyspareunia at later visits. Sexual
satisfaction increased from 98.0% at enrolment to
99.9% at 2 years among the controls (P < 0.001),
but there was no trend in satisfaction among
circumcised men (enrolment 98.5%, 2 years 98.4%, P =
0.8).
CONCLUSION
Adult male circumcision does not adversely affect
sexual satisfaction or clinically significant function
in men.
|
"There
are limitations to the present study.
Questions regarding sexual desire or
satisfaction are, of necessity, subjective
and refer to the individual's
self-perception. The
questionnaire focused on difficulties
with sexual function and did not
ascertain more subjective aspects of
sexual satisfaction such as changes in
time to ejaculation, subjective
intensity of orgasm or the partner's
satisfaction with intercourse
[19]. Also, circumcision status could not
be completely concealed from the
interviewers so there is a theoretical
possibility that interviewer bias might
affect participant response. Understanding
how circumcision affects sexual pleasure
is important in formulating public health
messages to promote the acceptability of
circumcision as an HIVprevention strategy.
In KwaZulu Natal, South Africa, those men who thought that
circumcised men enjoy sex more than
uncircumcised men were seven times more
willing to be circumcised, and men who thought that
women enjoy sex more with circumcised
men were over five times more willing to
have the procedure [15]. [All
the men enrolled for the trial were
willing to be circumcised, so all were
predisposed to believe that
circumcision would have no
ill-effects.]... Thus, our
findings that circumcision had no adverse
effects on sexual satisfaction or function
are reassuring
and provide important information for
future programmes.
|
There were six measures,
- desire [Laumann
et al. found 12-16% of men "lacked interest
in sex"]
- difficulty with penetration
- difficulty with ejaculating
(nothing about premature ejaculation)
- pain on
intercourse/dyspareunia
- "a problem regaining
erection after ejaculation" (?)
- satisfaction (on a
4-point scale - but they reported only two,
satisfied or not satisfied. Why did they
fail to report what might have been a salient
difference?)
and the lowest measure in
anything was 98.4% Laumann
et al. found a 39-46% incidence of
sexual dysfunction in this age group in the US.
(Maybe we should all move to Uganda - it's a sexual
paradise!)
It seems their measures were
too crude to measure anything. Remember, this is
only a part of their study of circumcision and HIV,
and they didn't want to find that
circumcision harmed sexual satisfaction - as the
word "reassuring" implies.
Also
- The subjects were all
volunteers for circumcision. Those who enjoyed
having their foreskins would be much less likely
to volunteer.
- The subjects were all paid
(substantially, by local standards) to take part.
- The subjects were members of
another culture than the experimenters. What does
that culture say about e.g. telling people what
they want to hear? (It's pretty obvious that
someone who circumcised you thinks circumcision is
a good thing.)
- What does that culture say
about sexual satisfaction and how it is measured?
- What does that culture say
about admitting to sexual failures?
Already this null finding has
been reported around the world with headlines like
"Circumcision Good For Sex" (Modern Ghana),
"Circumcision Does Not Deter Men from Enjoying Sex"
(Dr Bruno's Blog) and "Study: Circumcision Does Not
Affect Sexual Satisfaction" (Fox News). Now watch
these studies of adult volunteers in Uganda being
used to "prove" that circumcising babies in the US
is harmless!
|
More research with an agenda
|
J
Sex Med. 2008 Nov;5(11):2610-22. Epub 2008 Aug
28
Adult male circumcision: effects on sexual function
and sexual satisfaction in Kisumu, Kenya.
Krieger JN, Mehta SD, Bailey
RC, Agot K, Ndinya-Achola JO, Parker C,
Moses S.
INTRODUCTION: Male circumcision is being
promoted for HIV prevention in high-risk heterosexual
populations. However, there is a concern that
circumcision may impair sexual function.
AIM: To assess adult male circumcision's effect
on men's sexual function and pleasure.
METHODS: Participants in a controlled trial of
circumcision to reduce HIV incidence in Kisumu, Kenya
were uncircumcised, HIV negative, sexually active men,
aged 18-24 years, with a hemoglobin >or=9.0 mmol/L.
Exclusion criteria included foreskin covering less
than half the glans, a condition that might unduly
increase surgical risks, or a medical indication for
circumcision. Participants were randomized 1:1 to
either immediate circumcision or delayed circumcision
after 2 years (control group). Detailed evaluations
occurred at 1, 3, 6, 12, 18, and 24 months.
MAIN OUTCOME MEASURES: (i) Sexual function
between circumcised and uncircumcised men; and (ii)
sexual satisfaction and pleasure over time following
circumcision.
RESULTS: Between February 2002 and September
2005, 2,784 participants [men
who
had all volunteered to be circumcised in the hope
it would protect them from HIV] were
randomized, including the 100 excluded from this
analysis because they crossed over, were not
circumcised within 30 days of randomization, did not
complete baseline interviews, or were outside the age
range. For the circumcision and control groups,
respectively, rates of any reported sexual dysfunction
decreased from 23.6% and 25.9% at baseline to 6.2% and
5.8% at month 24. [In other
words some other factor caused sexual dysfunction
to decrease over time, vastly more than
any difference circumcision might have made.]
Changes over time were not
associated with circumcision status. Compared
to before they were circumcised, 64.0% of circumcised
men reported their penis was "much more sensitive,"
and 54.5% rated their ease of reaching orgasm as "much
more" at month 24. [Yes, and
what did the men who were not circumcised
report? Since everybody's sexual dysfunction
decreased dramatically over the time of the
experiment, did the non-circumcised men's
sensitivity and/or ease of reaching orgasm also
increase?]
CONCLUSIONS: Adult male circumcision was not
associated with sexual dysfunction. Circumcised men
reported increased penile sensitivity [What
ever
became of "If I was any more
sensitive ..."?] and enhanced
ease of reaching orgasm. [Some
call it "enhanced ease of reaching orgasm", others
may call it greater tendency to premature
ejaculation.] These data indicate that
integration of male circumcision into programs to
reduce HIV risk is unlikely to adversely effect male
sexual function.
[Another paper flowing from
the same study, and therefore with the same
faults, gained worldwide headlines in April 2009:
Krieger, J; Mehta, S; Bailey, R; Agot, K;
Ndinya-Achola, J; Parker, C; Moses, S. Adult male
circumcision: effects on sexual function and
penile coital injuries. J Urol, suppl, 2009: 181,
4 ]
|
Morten Frisch writes in passing in his
rebuttal to the responses of Morris, Waskett and Gray to his studies showing circumcision impairs
sexuality:
|
... The questionnaires used to assess potential
sexual problems in the two cited randomized controlled
trials in Kenya and Uganda were not presented in
detail in the original publications.4,5
Rather than blindly accepting such findings as any
more trustworthy than other findings in the
literature, it should be recalled that a strong study
design, such as a randomized controlled trial, does
not offset the need for high-quality questionnaires.
Having obtained the questionnaires from the authors
(RH Gray and RC Bailey, personal communication), I am
not surprised that these studies provided little
evidence of a link between circumcision and various
sexual difficulties.4,5 Several questions
were too vague to capture possible differences between
circumcised and not-yet circumcised participants (e.g.
lack of a clear distinction between intercourse and
masturbation-related sexual problems and no
distinction between premature ejaculation and trouble
or inability to reach orgasm). Thus, non-differential
misclassification of sexual outcomes in these African
trials probably favoured the null hypothesis of no
difference, whether an association was truly present
or not.
|
|
Acta
Neurologica
Belgica 108: 90-93 (2008)
The effect of male circumcision on pudendal evoked
potentials and sexual satisfaction
M.G. Senol, B. Sen, K. Karademir, H. Sen, M.
Saracoglu
Circumcision is generally considered a simple, rapid
operation with medical benefits which accrue
throughout life. [The
authors are in Turkey.] The influence
of circumcision on sexual satisfaction has always
been
argued. In this study, the assessment of the
pudendal evoked potentials (PEP) in adults before and
at least 12 weeks after circumcision vas done. Healthy
males aged between 18-27 years, who were willing to
undergo circumcision were included in the study,
Before and after circumcision, sexual performance was
evaluated with the Brief Male Sexual Function
Inventory (BMSFI), consisting of sexual drive,
erection, ejaculation, problem assessment, and overall
satisfaction sections. Forty-three adult males were
enrolled in the study. Mean PEP latency was 41.97 +/-
0.25 (39.90-44.50) ms and 44.73 +/- 0.33 (40.90-47.60)
ms before and after circumcision, respectively. Mean
difference between pre- and postoperative PEP values
was 2.76 ms which was statistically significant (p
< 0.001). [But
significant of what? A long PEP - the time for
signals to go from the genitals to the brain - is
a symptom of erectile dysfunction.]
Mean ejaculatory, latency time was significantly
longer after circumcision (p < 0.001). In the light
of our findings, we conclude that circumcision may
contribute to sexual satisfaction by prolonging PEP
latency but further studies are warranted also
regarding the other dimensions of circumcision.
[References: 13]
[This is bizarre. These
doctors asked the men some questions about their
sexual satisfaction but don't mention the answers
(presumably non-significant, because they asked
the wrong questions) and jump to the conclusion
that circumcision is a Good Thing because of an
electrical measurement of the nerves!
In Turkey, men aged over 18
who had not been circumcised and were willing to
be, or needed to be, would be a very skewed sample
of the population. This is truly junk science. ]
|
Circumcision decreses glans senstivity
|
Zhonghua Nan Ke Xue. 2008 Apr;14(4):328-30
Circumcision affects glans penis
vibration perception threshold
[Article in Chinese]
Yang DM, Lin H, Zhang B, Guo W.
Abstract
OBJECTIVE:
To evaluate the effect of circumcision on the glans
penis sensitivity by comparing the changes of the
glans penis vibrotactile threshold between normal men
and patients with simple redundant prepuce and among
the patients before and after the operation.
METHODS:
The vibrotactile thresholds were measured at the
forefinger and glans penis in 73 normal volunteer
controls and 96 patients with simple redundant prepuce
before and after circumcision by biological vibration
measurement instrument, and the changes in the
perception sensitivity of the body surface were
analyzed.
RESULTS:
The G/F (glans/finger) indexes in the control and the
test group were respectively 2.39 +/- 1.72 and 1.97
+/- 0.71, with no significant difference in between (P
> 0.05). And those of the test group were 1.97 +/-
0.71, 2.64 +/- 1.38, 3.09 +/-1.46 and 2.97 +/- 1.20
respectively before and 1, 2 and 3 months after
circumcision, with significant
difference between pre- and post-operation (P
< 0.05).
CONCLUSION:
There is a statistic [significant?] difference in the
glans penis vibration perception threshold between
normal men and patients with simple redundant prepuce.
The glans penis perception
sensitivity decreases after circumcision.
|
Circumcision increased sexual dysfunction and difficulty
reaching orgasm
|
Andrologia. 2013 Apr 20. doi:
10.1111/and.12101. [Epub ahead of print]
Adult circumcision and male sexual health: a
retrospective analysis
Dias J, Freitas R, Amorim R, Espiridião P, Xambre L,
Ferraz L.
ABSTRACT
We aimed to evaluate possible associations of
circumcision with several sexual dysfunctions and to
identify predictors for the development of these
outcomes post-operatively. Telephone surveys about
sexual habits and dysfunctions before and after
intervention were conducted post-operatively to
patients that underwent circumcision in Centro
Hospitalar Vila Nova de Gaia/Espinho during 2011.
McNemar test was used for a matched-pairs analysis of
pre- and post-operative data. Odds ratios, adjusted in
a multivariate analysis, explored predictors of de
novo sexual dysfunctions after circumcision. With
intervention [circumcision],
there was an increase in
frequency of erectile dysfunction (9.7%
versus 25.8%, P = 0.002) and delayed
orgasm [as a sexual dysfuntion, i.e. trouble reaching orgasm]
(11.3% versus 48.4%, P < 0.001), and a significant
symptomatic improvement in patients with pain with
intercourse (50.0% versus 6.5%, P < 0.001).
Significant predictors for de novo erectile
dysfunction were diabetes mellitus (OR 9.81, P =
0.048) and lack of sexual desire (OR 8.76, P = 0.028).
Less than three sex partners (OR 7.04, P = 0.007) and
low sexual desire (OR 7.49, P = 0.029) were
significant predictors for de novo delayed orgasm.
|
Trimming residual
foreskin from cut men delays ejaculation
|
Mohammad Reza Namavar, Boroomand Robati1
Urology Annals, Saudi Urological Assn, Vol 3,
Issue 2, May 2011
Abstract:
Premature ejaculation (PE) is the most
prevalent sexual dysfunction in every country.
There are many types of treatment, but the main
limitation of medical treatment for premature
ejaculation is recurrence after withdrawal of
medicine. The
prepuce is a specific erogenous zone that
contains a rich and complex network of nerves.
Circumcision radically desensitizes the
penis, but incomplete
circumcision may cause premature ejaculation. We
evaluate the effect of removal of foreskin
remnants in adults on PE....
...
The abundance of myelinated and
nonmyelinated nerve fibers explains the
high sensitivity of the human foreskin and
its function as erogenous tissue.
...
Circumcision
removes more than 50% of the skin and mucosa
from the penis. (citing CIRP.org)
...
Removal of
foreskin remnants in adults significantly
decreased penis sensitivity.
...
The frequency of intercourse per week
significantly increased after treatment [suggesting the
men were enjoying sex less, and hence
needed to do it more].
[While this study claims that it is the
foreskin remnants cause PE, it is more
likely that removal of any of the foreskin
caused the PE in the first place, and that
removal of the remnants of the foreskin
merely makes it more difficult to reach
orgasm and ejaculation at all. Intravaginal
latency
ejaculatory time (IVELT) increased from
64.25 seconds to 731.48 seconds, but
they (of course) give no baseline IVELT
for intact men - which is under much
more control because of feedback from
the foreskin.]
|
Intact men are happier to be intact than
men cut as babies or children are happy to be cut
Arch Sex Behav
DOI 10.1007/s10508-017-1064-8
Attitude Toward One’s Circumcision Status Is More
Important than Actual Circumcision Status for Men’s
Body Image and Sexual Functioning
Jennifer A. Bossio, Caroline F. Pukall
Abstract Research exploring the impact of
circumcision on the sexual lives of men has failed to
consider men’s attitudes
toward their circumcision status, which may, in part,
help to explain inconsistent findings in the literature.
The current study explored the potential relationship
between attitudinal factors toward one’s circumcision
status, timing of one’s circumcision, and sexual
correlates. A total of 811 men (367 circumcised as
neonates,107 circumcised in childhood, 47 circumcised in
adulthood, and 290 intact) aged 19–84 years
(M=33.02,SD=12.54) completed an online survey.We
assessed attitudes toward one’s circumcision status,
three domains of body image (Male Genital Image Scale,
Body Exposure during Sexual Activities Questionnaire,
Body Image Satisfaction Scale), and self-reported sexual
functioning (International Index of Erectile Function).
Men who were circumcised as adults or
intact men reported higher satisfaction with their
circumcision status than those who were circumcised
neonatally or in childhood. Lower satisfaction
with one’s circumcision status—but not men’s actual
circumcision status—was associated with worse body image
and sexual functioning. These
findings identify the need to control for attitudes
toward circumcision status in the study of sexual
outcomes related to circumcision. Future
research is required to estimate the number of men who
are dissatisfied with their circumcision status, to
explore the antecedents of distress in this
subpopulation, and to understand the extent of negative
sexual outcomes associated with these attitudes.
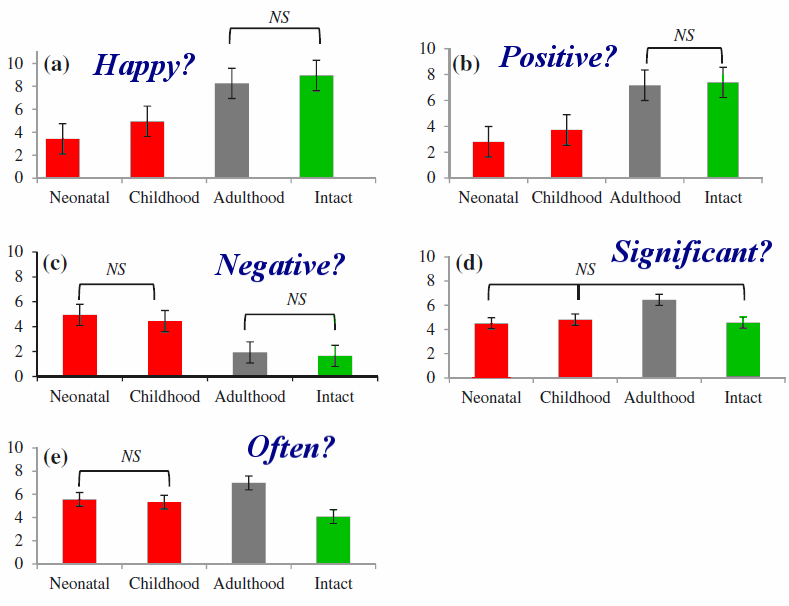
Fig. 1 Mean responses to questions assessing
men’s satisfaction with their own circumcision status.
Note. Group means are significantly different unless
otherwise specified with NS (nonsignificant). Error bars
represent standard error. Y-axis represents participant
response from 0 reduce the excessive
spacing between words [to 10 on five
measures (] happy/positive/negative/important/often),
where 5 represents neutral. X-axis represents
circumcision status group.
a How happy are you with your circumcision status?
(Happy).
b How much is your circumcision status a positive issue
for you in everyday life? (Positive).
c How much is your circumcision status a negative issue
for you in everyday life? (Negative).
d How much do you think about your circumcision status
as a significant part of who you are? (Significant).
e How often do you think about your circumcision status?
(Often)
[a. Intact men are significantly more happy to
be intact than non-consented cut men are to be cut.
b. Intact men's status is significantly more
positive for them than non-consented cut
men's.
c. Non-consented cut men's status is
significantly more negative for them than
intact men's.
d. Adult-cut men think about their status as a
significant part of who they are.
e. Intact men think about their status less often
(and adult-cut men more often) than non-consented
cut men.
Men cut as adults may have really needed it and
benefited from it, or wanted it and be happy to get
what they wanted.]
Discussion
Men’s Attitudes Toward Their Circumcision Status
Exploration of the descriptive statistics revealed
that—for a substantial proportion of men in this
sample—circumcision status was not a negative or
important issue. In fact, men in this sample who
underwent circumcision as adults or intact men
reported high levels of satisfaction with their
circumcision status. [It
is bizarre to see these two diametrically
opposite groups being lumped together.]
However, there was a subgroup
of men for whom their circumcision status was
highly distressing, and these men were more likely
to have been neonatally circumcised. One
possible explanation for the high levels of distress
among some circumcised men, and the relative
importance of one’s self-reported happiness with
their circumcision status, is the role of choice in
their circumcision status. [Possible?
Of course it is!] The issue of choice
in neonatal circumcision has been the center of a
heated debate (Earp, 2015; McMath, 2015; Svoboda,
Van Howe, &Dwyer, 2000). Perhaps this finding
is, in part, reflective of the fact that men who
were not neonatally circumcised were able to rectify
dissatisfaction with their circumcision status by
undergoing circumcision. On the other hand,
circumcised men have far fewer options to reverse
their circumcision status,and the options that are
available to them (e.g., foreskin ‘‘restoration’’;
Hammond, 1999) are timely [apparently meaning
"time-consuming"], labor-intensive, and never truly
‘‘restorative’’ (because the nerve fibers lost to
circumcision cannot be re-grown).
Future research is needed to obtain an accurate base
rate estimation with respect to the frequency that
men fall into the category of ‘‘distressed’’over
their circumcision status, as this reaction to one’s
circumcision status—among others—should be addressed
in future public policy statements about
circumcision. In a recent study exploring genital
dissatisfaction in a national sample of U.S. men
aged 18–65 (Gaither et al., 2017), 7% of the
3996 participants who answered the genital
satisfaction questions reporte ddissatisfaction with
their circumcision status, 62% reported
satisfaction, and 31% reported neutral satisfaction.
Dissatisfaction was determined by a score of 1, 2,
or 3 on a seven point scale, satisfaction was 5,
6,or 7, and a score of 4 was considered neutral. It
should be noted, though, that actual circumcision
status was not assessed in Gaither et al.’s national
survey [which makes it
worthless].
Similarly, it appears that the number of men who
reported feeling unhappy with their circumcision
status was a minority in the current study,
regardless of timing of circumcision status [but
not if timing was regarded].
Interestingly, observed effect sizes for group
differences ranged from large (e.g., Happy,
Positive) to medium (Negative, Significant,Often)
suggesting that, at least within the current sample,
attitudes toward one’s
circumcision status vary greatly across
circumcision status. [This
ought to be self-evident. Compare attitudes
towards one's amputation status: people with
feet cut off are more likely to be unhappy about
it than people with feet.] However,
even small group differences would be theoretically
relevant in this case, as this study is the first to
document that the life stage at which one undergoes
circumcision is associated with the level of
dissatisfaction toward one’s circumcision status in
a subsample of men. Understanding the antecedents of
this dissatisfaction is needed to elucidate what
separates the distressed group from the neutral or
satisfied men (e.g., reason for circumcision, mental
health correlates such as depression, anxiety, body
dysmorphia, social comparison) with the intent of
decreasing distress related to circumcision status. [Wow! Way to ignore the
Elephant In The Room! Cut men hate being cut
when it was an unnecessary reductive imposition
on them, and not so much when they were thought
to need it, actually needed it, or wanted it.]
| Table 2
Participants who reported feeling ‘‘unhappy’’ or
‘‘neutral/happy’’ toward their circumcision
status, broken down by timing of circumcision |
|
Unhappy n (%) |
Neutral/happy n (%) |
| Neonatally circumcised |
235 (64.2) |
131 (35.80) |
| Circumcised as child |
45 (42.5) |
61 (57.5) |
| Circumcised as adult |
6 (12.8) |
41 (87.2) |
| Intact |
16 (5.5) |
270 (94.4) |
| Data were missing for
5 individuals |
[These figures are entirely
comparable with other
self-selected polls. The results might be
even more dramatic if we could see what
proportion were actually happy, and not just
neutral. As it is, a clear majority of a
moderately large sample of neonatally cut men
are unhappy with their status. A very large
majority of intact men are neutral or happy to
be intact. The overall ratio is thirty
to one!]
Bossio and Pukall treat
dissatisfaction with being genitally cut as a mere
variable in studies of sexual function, not as an
issue in itself, and to a large extent, like
many pro-cutters before them, treat dis/satisfaction
with being intact as equivalet to dis/satisfaction
with being genitally cut - as though the fact of
being cut without consent was not itself an issue -
while dissatisfaction with being intact arises
indirectly, e.g. from being different from others
(and even being bullied by them for being intact),
or some abnormality of the foreskin.
|
Archives
of
Sexual Behavior
https://doi.org/10.1007/s10508-018-1180-0
LETTER TO THE EDITOR
Antecedents of Emotional Distress and Sexual
Dissatisfaction
in Circumcised Men: Previous Findings and Future
Directions—Comment on Bossio and Pukall (2017)
Tim Hammond, Mark D. Reiss
Received: 29 September 2017 / Accepted: 21 February 2018
© Springer Science+Business Media, LLC, part of Springer
Nature 2018
Bossio and Pukall (2017) make an important contribution
by identifying the subpopulation of men distressed by
having been circumcised nontherapeutically as infants or
children. This group, heretofore largely overlooked, has
been recognized for decades by grassroots citizens
concerned about risks, harms, and disadvantages of
culturally motivated genital cutting.
We agree that “Future research is
required to…explore the antecedents of distress in
this subpopulation.” Although earlier explorations of
such antecedents were reported, those surveys relied
on self-selecting samples and should be regarded as
preliminary (Hammond, 1999; Hammond & Carmack,
2017). Even so, serious and even debilitating distress
over having been circumcised in infancy has now been
described in several reports (Earp & Darby, 2017).
Based on available data, such distress can be caused by
physical damage, including excessive skin removal
causing tight, painful erections; meatal stenosis;
prominent or irregular scarring; numb, hypersensitive or
painful scars; unsightly scar pigmentation; painful skin
bridges; gouges in and/or toughening of the glans; and
other issues. Extensive photographic evidence of
physical damage submitted by Hammond’s respondents is
viewable at www.CircumcisionHarm.org.
Sexual distress may be caused by, among other variables,
insufficient skin mobility for self-pleasuring or ease
of vaginal/anal penetration; loss of mechanical
lubrication, reduced seminal fluid preservation,
inability to achieve sufficient stimulation from vaginal
intercourse to reach orgasm (causing respondents to
resort to anal, oral, manual or artificial stimulation);
premature/delayed orgasm; and erectile dysfunction
perceived as attributable to circumcision.
Still others endure psychological, emotional, and
selfesteem issues subsequent to acquiring knowledge
regarding the significant loss of erogenous tissue
(Earp, Sardi, & Jellison 2018); elimination of the
foreskin’s valuable protective, sexual, and
immunological functions (Fleiss, Hodges, & VanHowe
1998); and one’s lack of choice and control in
determining how much of their genitals they were
permitted to keep.
These circumcision sufferers often express a deep sense
of having been damaged or mutilated; feelings of
compromised masculinity or shame; depression; addictive
behaviors; alexithymia; and body eudysmorphia [meaning true
dysmorphia where the body itself is distorted] (Watson
& Golden, 2017). Others describe feelings of
violation of their basic human right to bodily integrity
and autonomy through medical, religious, and
governmental neglect; a breakdown in sexual intimacy;
betrayal by parents and medical professionals; and
compromised relationships with family, friends, and
others who discount or ridicule their pain. Others
experience suicidal ideation and/or attempts.
Previously published books exploring the disadvantages
and harm of nontherapeutic newborn circumcision
(Goldman, 1997; Watson, 2014) and proliferating social
media outlets (Foregen, 2017; I Am Not Thankful, 2017;
Men Do Complain, 2017; National Organization of
Restoring Men, 2017; Personal Accounts of Circumcision
Resentment, 2017) provide a broad and deep foundation
for more empiricalresearch.
Moreover, specific guidelines for exploring longterm
adverse physical, sexual, and mental health effects of
newborn circumcision may be found in Hammond’s two
surveys. Caution, however, is warranted in drawing too
many conclusions from quantitative analyses. Researchers
must also listen to the lived experiences of this
subpopulation.
Since an estimated 30% of the world’s males were
subjected to nontherapeutic circumcision as newborns or
children (U.N. International NGO on Violence Against
Children, 2012), the scope of this problem could be
significant and will surely grow as knowledge about
foreskin anatomy, development, and physiology becomes
more easily accessible with the expansion of the
Internet.
Even without further research into this subpopulation,
we support Bossio and Pukall’s recommendation that
“…this reaction to one’s circumcision status—among
others—should be addressed in future public policy
statements about circumcision.” |
Which do women prefer?
|
I studied in North America at University, once
arriving at the University and living in halls, with
the English accent and dry humour, I did pretty well
with the lady's. However, once the word went round,
like wild fire, that I was 'uncut', I have never had
so much action in my life, I had girls coming up to me
in bars, in the cafeteria, and they couldn't stop
examining it! I didn't complain the 1 year exchange
was the happiest time of my life!
- scott, cornwall, UK, in the Daily Mail, January 27, 2012
-
|
Three studies have addressed this question, and come to
opposite conclusions. All were flawed.
- The O'Hara and O'Hara
study in the UK was a self-selected, voluntary survey. Some of
its subjects were recruited from anti-circumcision sources,
tending to bias results away from circumcision, but it had two
strikes in its favour.
- All the women who took part had experienced sex with
both intact and circumcised men.
- They described in detail what they experienced, and
sometimes found favourable attributes in spite of their
preferences
|
"[The] women [who] preferred circumcised
partners ... still found unaltered partners to
evoke more vaginal
fluid production, a lower vaginal discomfort
rating and fewer complaints ...
during intercourse than their circumcised
partners."
"Respondents overwhelmingly concurred that the
mechanics of coitus was different for the two
groups of men. Of the women, 73% reported that
circumcised men tend to
thrust harder and deeper, using
elongated strokes, while unaltered men by
comparison tended to thrust more gently, to
have shorter thrusts, and tended to be in
contact with the mons pubis and clitoris more,
according to 71% of the respondents."
|
So its results have qualitative if not quantitative merit.
The O'Hara study - like these pages - is written from the
point of view that intactness is normal, which may look like
an anti-circumcision bias in the prevailing pro-circumcision
climate. The authors have developed their findings into a
book, Sex As Nature
Intended It.
- The Williamson and Williamson study
in Iowa was a cohort study, but it had a very high (46%)
non-response rate, tending to bias the results in an unknown
way. The women had all just delivered sons, further biassing
the study away from the entire female population. [August
25, 2010: Truth will out. At least one of the women had just had a daughter
but when she said if she had had a son she would have had
him circumcised, she was invited to take part.]
Its faults are serious:
- Only 16.5% of those who answered had experienced sex
with both intact and circumcised men.
- Some of their responses were irrational, suggesting they
didn't know what they were talking about:
- 77% said circumcised penises "seemed more natural"
- 54% said circumcised penises "stayed softer"
Predictibly, a majority of the women preferred circumcised
penises for sex, but interestingly, that majority (71% for
vaginal intercourse) was lower than the proportion
(78%) who had never known anything else.
The Williamsons' study is written with a clear
pro-circumcision bias. It assumes that a mother's sexual
preference is a reasonable basis on which to decide
whether to cut part off her son's genitals. (Consider if
the sexes were reversed!)
- A random controlled study, but from a a dubious source.
SEXUAL SATISFACTION OF WOMEN PARTNERS OF
CIRCUMCISED MEN IN A RANDOMIZED TRIAL OF MALE
CIRCUMCISION IN RAKAI, UGANDA
IAS Conf HIV Pathog Treat 2009
Jul 19-22;5th: Abstract No. MOPDC104
G. Kigozi, I. Lukabwe, M. Wawer, D. Serwadda, F.
Nalugoda, J. Kagayi, N. Kiwanuka, F. Mangen
Wabwire, T. Lutalo, D. Nabukenya, G. Kigozi
Nalwoga, R. Gray
BACKGROUND: Some activists
have objected to male circumcision
because of the lack of data on female sexual
satisfactions and sociologists have urged that
circumcision roll out programs consider social
factors that may affect women, including female
sexual satisfaction. There has also been
speculation that removal of the foreskin reduces
female sexual satisfaction because the gliding
action of the foreskin is thought to facilitate
vaginal penetration. We assessed the effect of
adult medical male circumcision on postoperative
female sexual satisfaction.
METHODS: We investigated self-reported sexual
satisfaction among 455 women partners of men
circumcised in a randomized trial of male
circumcision for HIV prevention in Rakai, Uganda.
Women aged 15-49 were interviewed about their
sexual satisfaction before and after their
partners were circumcised. We analyzed female
reported changes in sexual satisfaction using
Chi-square or Fisher's exact tests.
RESULTS: Only 2.9%
(13/455) of women reported less sexual
satisfaction after their partners were
circumcised. 57.3% (255/455) reported no change in
sexual satisfaction and 39.8% (177/455) reported
an improvement in sexual satisfaction following
their partners' circumcision. There was no
statistically significant difference in reported
change in sexual satisfaction before and after
partner's circumcision by age, religion and
education status.
CONCLUSIONS: The overwhelming
majority of women (97.1%) report either no change
or improved sexual satisfaction after their male
partner was circumcised. These findings suggest
that male circumcision has no deleterious effect
on female sexual satisfaction.
[Why add "no change" to
the satisfied? Putting the opposite spin on
it, the majority of women, 58.9% (268/455)
report no improvement in sexual satisfaction.
It is clear from the
wording what outcome the researchers wanted.
There could be no blinding of the results or
placebo control. This abstract does not give
before and after figures, but a
study of men by the same researchers -
who have produced several papers all
supporting circumcision - found no difference
because satisfaction approached 100% both
before and after. This raises the question, in
each group, how good was it before, and how
good after. What if the 39.8% experienced
marginal improvement while the 2.9% suffered
catastrophic losses?]
|
|
The Canadian journal of human
sexuality 08/2015; 24(2).
DOI: 10.3138/cjhs.242-A2
You either have it or you don’t: The impact of male
circumcision status on sexual partners
Jennifer A. Bossio, Caroline F. Pukall, and Katie
Bartley
This study was an exploration of the impact of men’s
circumcision status on their sexual partners, focusing
on sexual functioning, sexual satisfaction, general
preferences for circumcision status, and beliefs about
circumcision status. A total of 196 individuals (168
women, 28 men) currently in a sexual relationship with a
man were recruited for an online survey. Sexual
functioning for female or male participants (assessed by
the FSFI or IIEF-MSM, respectively) was not impacted by
circumcision status, but women
with intact partners reported higher levels of sexual
satisfaction, while no differences were
observed in the male sample. Women’s responses indicated
that circumcision status minimally impacted satisfaction
with partner’s genitals, while men
with
intact partners indicated significantly higher levels
of satisfaction than those with circumcised partners.
Overall, women and men rated high levels of satisfaction
with their partner’s circumcision status and did not
wish for it to change. Women indicated a slight
preference for circumcised penises for vaginal
intercourse and fellatio, and held more positive beliefs
about circumcised penises, while men indicated a strong
preference toward intact penises for all sexual
activities assessed and held more positive beliefs about
intact penises. The current study demonstrates distinct
gender differences in attitudes toward circumcision
status but minimal impact of circumcision status on
sexual functioning. Future research should further
explore sexual correlates of circumcision status, with a
focus on directionality of said correlates and the
impact on couples, as well as replicating the findings
with a larger sample, specifically with respect to the
male sample.
...
Eligible participants met the following criteria: (i)
over the age of 18; (ii) able to read and write English
fluently; and (iii) in a sexual relationship with a
cisgendered (i.e., biologically born) male partner for
at least the past 3 months. Participants were excluded
based on the following criteria: (i) if they or their
partner were circumcised as an adult, or circumcised
to
correct
a medical condition (e.g., phimosis); (ii) if
they or their partner had any anatomic or medical
abnormalities of the penis (e.g., complications
during circumcision, hypospadias, genital
modifications such as piercings); and (iii) if
their partner had a diagnosis of a sexual dysfunction.
[So two of the main groups who
might have made genital cutting look worse were
excluded before the study began! ]
A total of 196 individuals who met eligibility criteria
completed the study in full, 168 women and 28 men.
[The experience of sex with a man is of course very
different for men and women.]
76 (45.2%) of the women's partners were
intact, 14 (50%) of the men's.
[The study did not record the effect of genital
cutting on the cut men themselves, but on their
partners. (Imagine for a moment a study of
female cutting the asked only the cut women's
partners about their experiences.)]
Women with intact partners reported significantly
higher levels of sexual satisfaction than women with
circumcised partners
...
The observation that women with intact partners
endorsed higher sexual satisfaction ratings on the
F[emale ]S[exual ]F[unction ]I[ndex] is interesting,
considering that women’s responses to other subsections
of this survey indicated a preference for circumcised
penises (e.g., higher self-report satisfaction with
their partner’s flaccid penis compared to women with
intact partners, higher preference for circumcised penis
during some sexual activities, more positive beliefs
about circumcised penises). It
is possible that the presence of foreskin provides
some benefits to sexual satisfaction outside of the
domains assessed by the FSFI. Additional
research is required to clarify the nuanced role of
foreskin in sexual intercourse and partner
enjoyment/sexual satisfaction, particularly among women.
|
Here is one woman's story.
The underlying fact is that women prefer what they are familiar
with. But regardless of what a woman prefers, this should not be
a consideration for circumcising a baby boy because
- He might grow up to be celibate
- He might grow up to be gay
- The majority preference might have changed by the time he
grows up
- His future partner might not share the majority preference
- Forcibly cutting part off one person to suit another
(hypothetical, unknown) person is unethical
- His preference should be overriding. (Imagine trying
to justify circumcision of girls to suit men's
preferences in the Western world today...)
If a man chooses to be circumcised to please his wife, that's
his decision - but read on.
Who can compare them?
It is impossible for any man to both have been circumcised in
infancy and left intact; any studies must compare different men.
Two groups of men have some experience of both having and not
having a foreskin, though:
- Men circumcised in adulthood
Their reactions vary widely. One problem is that some of the
most vocal proponents of circumcision from this group chose to
be circumcised for sexual reasons - they already had a sexual
investment in having a circumcised penis. Others had physical
problems with their foreskins that were solved by
circumcision. In general, reports from those who were
circumcised in adulthood for non-sexual reasons take a
negative view of the outcome.
|
Back
in
1964, ...
I was serving a tool and die apprenticeship in a
machine shop with several men that had served in
the military during WWII. They shared their
experiences with having been circumcised as
adults. They were both circumcised when they found
themselves in military hospitals during the war.
One thought of it as a really good thing before it
was done, (It would be a status symbol because
both men came from a small coal mining town, and
only the wealthy were born in hospitals, and even
then, only some of them were circumcised), but he
felt very much differently about it afterwards.
The second man would not have wanted it done, but
he was too sick to give his view on it before the
operation. ...
Both commented that their losses were very
significant (one said he experienced a 70% loss of
feeling, and the other said he had lost about 3/4
of his). You have to realize that this was only
their opinions, and not the result of some
measurement. Still, I find the similarities in
numbers very interesting.
The man that would have objected tossed in one
other insight. He mentioned that masturbation was
almost a complete loss. He commented that you
could still do it of course, but that it had been
stripped of its main pleasures. He said you could
do it "to scratch an itch", but it was mostly work
until he would orgasm, which he said was pretty
much the same as before. The other thing that he
mentioned was that now he needed either a pinup
picture, or a "girly" magazine to get it to work,
where he never had to use any props before. ...
- John Soemer
December 11, 2005
|
As mentioned above, the effects on the nervous system of
adult circumcision are different from those of infant
circumcision. The circumcised boy also experiences the whole
development of his sexuality with a circumcised penis - he
learns to use what he's got. A man circumcised in adulthood
has to relearn, and may be unable to do so.
|
You do lose an enormous amount of sensitivity. It
has no effect on ejaculation, or whether you can
get an erection or not. Because you lose so much
sensation you have to work much harder to get the
same sensation which affects sex completely.
Performance artist Peet Pienaar,
who filmed and exhibited his own circumcision in
2000
|
His view is interesting because his reason for getting
circumcised is neither medical nor sexual (and if it was
covertly sexual, he presumably expected an
improvement).
These men responded within a few hours of a contrary article
being published:
-
|
J
Urol 2002 May;167(5):2113-2116
Adult Circumcision
Outcomes Study:
Effect on Erectile Function, Penile
Sensitivity, Sexual Activity and
Satisfaction
Fink KS, Carson CC,
DeVELLIS RF. Robert Wood Johnson Clinical
Scholars Program and Division of Urology, School
of Medicine, and the Department of Health
Behavior and Health Education, School of Public
Health, University of North Carolina at Chapel
Hill, Chapel Hill, North Carolina.
PURPOSE: Evidence
concerning the effect of circumcision on sexual
function is lacking. Men circumcised as adults
are potentially in a unique position to comment
on the effect of a prepuce on sexual
intercourse. We examine sexual function outcomes
in men who have experienced sexual intercourse
in the uncircumcised and circumcised states.
MATERIALS AND METHODS:
Men 18 years old or older when circumcised were
identified by billing records during a 5-year
period at an academic medical center. Medical
charts were reviewed for confirmation of the
procedure and to identify the indication(s).
These men were surveyed to assess erectile
function, penile sensitivity, sexual activity
and overall satisfaction. Data were analyzed
using paired t tests to compare category scores
before and after circumcision.
RESULTS: A total of
123 men were circumcised as adults. Indications
for circumcision included phimosis
in 64% of cases, balanitis
in 17%, condyloma
in 10%, redundant
foreskin in 9% and elective in 7%. The response
rate was 44% among potential responders. Mean
age of responders was 42 years at circumcision
and 46 years at survey. Adult circumcision
appears to result in worsened
erectile function (p = 0.01), decreased
penile sensitivity (p = 0.08), no
change in sexual activity (p = 0.22) and
improved satisfaction (p = 0.04). Of the men 50%
reported benefits and 38% reported harm.
Overall, 62% of men were satisfied with having
been circumcised.
[Presumably
this means 12% reported no change, and they
were counted among the satisfied.
Considering that the 64% who were
circumcised for phimosis would have expected
sexual benefits, this is a remarkably poor
success rate.]
CONCLUSIONS: Our
findings may help urologists better counsel men
undergoing circumcision as adults.[Notice
how
circumcision is taken as a given. What these
findings should do is encourage urologists
to seek alternatives to circumcision.]
Prospective studies are needed to better
understand the relationship between circumcision
and sexual function. [And
before they do that, studies are needed to
better understand the relationship between
the foreskin and sexual function,
but this is something they don't seem to
want to think about.]
PMID: 11956453 [PubMed - as
supplied by publisher]
|
A small survey of men circumcised as
adults finds detriment
|
09
Does circumcision improve couple's sexual life?
I. Solinis, A. Yiannaki
|
|
I. Solinis
Department of Urology,
General Hospital of
Didimoticho, Didimoticho,
Greece
A. Yiannaki
Department of Urology,
General Hospital of
Didimoticho, Didimoticho,
Greece
|
Background: The aim of the study was to
compare sexual life and enjoyment of men (and
their partner) that were circumcised as adults
before and after their circumcision. Methods: The
study included 123 sexually active men that were
circumcised two years before or more. [The
effect of circumcision on a man's sex life
depends on why he was circumcised. If it was
for a sex-related problem, an improvement is
to be expected.] The mean age was
36 years (22- 64). All the men filled a
questionnaire about the quality of their sexual
life and the sexual enjoyment before and after
circumcision. Also, there were questions about
partner's sexual life improvement. The results are
presented below.
Results: 16% answered that their sex life
was improved, while 35%
reported a worse sex life after
circumcision. There were no significant
differences in erection and ejaculation.
|
65% reported that the ejaculation latency time
increased significantly after circumcision but
only 10% of them reported that this fact improved
sexual life. 46% of men reported that their
partner's sexual life worsened after circumcision,
33% reported that their partner's sexual life
improved and 21% reported no significant
difference. [Men's
reporting of women's sexual satisfaction is
notoriously inaccurate.]
Conclusion: There was a decrease in
couple's sexual life after circumcision indicating
that adult circumcision adversely affects sexual
function in many men or/and their partners,
possibly because of complications of surgery and
loss of nerve endings. The results support the
view that physicians and parents should be
informed of the potential benefits and risks
before newborns are circumcised. [The
results support the view that newborns
should not be circumcised.]
journal of men's health &
gender
Vol. 4, No. 3, pp. 357-378, September 2007 361
|
Circumcised men are more likely to have premature
ejaculation
|
Prevalence
and Correlates of Premature Ejaculation in a
Primary Care Setting: A Preliminary
Cross-Sectional Study
Wei Shuong Tang, MMed and Ee Ming Khoo, MD
Kuala Lumpur, Malaysia
DOI: 10.1111/j.1743-6109.2011.02280.x
ABSTRACT
Introduction. Premature ejaculation (PE)
is common. However, it has been underreported and
undertreated.
Aims. To determine the prevalence of PE
and to investigate possible associated factors of
PE.
Methods. This cross-sectional study was
conducted at a primary care clinic over a 3-month
period in 2008. Men aged 18–70 years attending the
clinic were recruited, and they completed
self-administered questionnaires that included the
Premature Ejaculation Diagnostic Tool (PEDT),
International Index of Erectile Function,
sociodemography, lifestyle, and medical illness.
The operational definition of PE included PE and
probable PE based on the PEDT.
Main Outcome Measure. Prevalence of PE.
Results. A total of 207 men were recruited
with a response rate of 93.2%. There were 97
(46.9%) Malay, 57 (27.5%) Chinese, and 53 (25.6%)
Indian, and their mean age was 46.0 ± 12.7 years.
The prevalence of PE was 40.6% (N = 82) (PE:
20.3%, probable PE: 20.3% using PEDT). A
significant association was found between
ethnicity and PE (Indian 49.1%, Malay 45.4%, and
Chinese 24.6%; chi2 = 8.564, d.f. = 2,
P = 0.014). No significant association was found
between age and PE. Multivariate analysis showed
that erectile dysfunction (adjusted odds ratio
[OR] 4.907, 95% confidence interval [CI] 2.271,
10.604), circumcision
(adjusted OR 4.881, 95% CI 2.346, 10.153),
sexual intercourse <= 5 times in 4 weeks
(adjusted OR 3.733, 95% CI 1.847, 7.544), and
Indian ethnicity (adjusted OR 3.323, 95% CI 1.489,
7.417) were predictors of
PE.
Conclusion. PE might be frequent in men
attending primary care clinics. We found that
erectile dysfunction, circumcision,
Indian ethnicity, and frequency of sexual
intercourse of <= 5 times per month were
associated with PE. These associations
need further confirmation.
Tang WS and Khoo EM. Prevalence and correlates of
premature ejaculation in a primary care setting: A
preliminary cross-sectional study. J Sex Med
**;**:**–**.
|
- Men who have restored
their foreskins
The same objection can be made, that men who restore do so for
sexual reasons (though some do so more as a political
statement, to get back what they feel was taken unjustly, and
find new sexual pleasures to be a bonus). Further,
non-surgical restoration is time-consuming and requires
dedication, so those who complete the process are strongly
motivated. Even then, restoration can never hope to replace
all that was lost. In spite of this, there are clear
differences in quality: restored men report good sensations
from the movement of their secondary foreskins, and increased
sensitivity from their covered, de-keratinised glanses.
- Gay men
Gay men are in a unique position to compare intact and
circumcised penises, being likely to have experience of both
kinds, and first hand experience of one kind or the other.
(Intact men are especially likely to notice the difference.)
No consensus has emerged, but some magazines cater especially
to a taste for intact men, and erotic fiction - presumably
market-driven - almost invariably includes them. A growing
genre of gay erotic videos is made in Central Europe,
featuring all-intact casts. This has been badmouthed as a
"fetish", but it is the preference
for an amputation over the whole body part that is in
every other case considered the fetish, and a rather bizarre
one.
Intact gay men typically report that their circumcised
partners are "too rough" and circumcised gay men that their
intact partners are "too gentle" (untill they are taught),
strongly confirming the suggestion that circumcision reduces
sensitivity.
Docking
One practice, "docking", "snoodling" or "frontage" (one
man's glans inside another's foreskin), is only possible
between men, at least one of whom is intact. "Double
docking" (one foreskin inside another) is only possible when
both are intact. While few parents would choose to leave
their son intact just in case he grows up to want to dock,
he is hardly going to thank them for removing that option if
he does. Circumcising him will not of course prevent him
from growing up gay, nor prevent him from docking if he does
- he will just have to find intact men do to it with.
(Heterosexual couples - if the man is intact - may enjoy
foreskin-nipple-, foreskin-clitoris-, foreskin-tongue- or
just foreskin-finger-play, too.)
Sex manuals for gay men written by circumcised men have a
hard time coping with docking: they can't deny that at
least one foreskin is essential, so they downplay the
whole thing, saying such things as "the pleasure is more
psychological than physical" - whatever that might mean.
|
A Docking Aid
Topco Sales
manufactured "The Docker", a cylinder of
gel-plastic for two men to insert their penises
from opposite ends:
"Whether you're cut or uncut, you can enjoy the
sensation of docking with your partner!"
"Smooth, soft, realistic Cyberskin®
feels like real foreskin."

Like the Manhood, the existence of such a toy
underlines what is lost by circumcision. (The
product no longer seems to be available, but a very similar one,
enabling two men to touch penises - without
reference to foreskins or docking - is.)
|
The Foreskin and fertility
|
New Scientist Daily News June 5,
2008
Male circumcision is a weapon in the sperm wars
By Kurt Kleiner
Circumcision and other forms of male genital
mutilation have always been a puzzle. The ritual
mutilations can leave the man vulnerable to infection
and even death. So why do some societies insist on
such a risky ritual for their men?
There may be an evolutionary explanation, according
to Christopher Wilson, of Cornell University in New
York, US. It could function to reduce a young man’s
potential to father a child with an older man’s wife,
he says.
Sperm competition theory predicts that males will
evolve ways to ensure that their sperm, and not
another male’s, fertilises a female’s eggs. Genital
mutilation, in this view, is just another way to win
the sperm war.
In some forms of mutilation, the handicap to sperm
competition is obvious. There is subincision, for
example, where cuts are made to the base of the penis.
This causes sperm to be ejaculated from the base
rather than the end, and is performed in several
Aboriginal Australian societies, says Wilson.
In some African and Micronesian cultures, young men
have one of their testicles crushed.
Male genital mutilation makes it less likely that a
male will manage to father a child with another man’s
wife, Wilson says.
Home advantage
Circumcision is one of the less painful forms of
mutilation [This is, to say
the least, debatable], but it is also
less effective at reducing sperm competition. Wilson
suggests, however, that the lack of a foreskin could
make insertion or ejaculation slower, meaning brief,
illicit sex is less likely to come to fruition and
lead to a pregnancy.
Younger men, he says, willingly submit to having
their reproductive ability reduced because they
benefit socially from the older men, by forming
alliances, and by gaining access to weapons or tribal
lore.
The older men have also gone through the ritual, and
seen their own reproductive effectiveness reduced. But
if a man with, say, four wives wants to ensure that
any children his wives produce are his, there is
pressure to make sure other men can’t successfully
impregnate them.
The husband’s own reproductive ability is impaired,
but continuous and repeated access to his wives makes
up for it, while any genital mutilation is a greater
handicap to an interloper trying to sneak brief
occasional sex with his wives.
...
Wilson has now tested the idea. If the sperm
competition theory is correct, he reasoned, then male
genital mutilation should be more common in societies
where men tend to have multiple wives, especially
those in which the wives live apart from the husband.
The mutilation would also probably be carried out in
a public setting, witnessed mostly by other men, and
performed by a non-relative. Men who refused would
face social sanctions.
Who’s the daddy?
Wilson searched anthropological databases and found
that his predictions were borne out: 48% of highly
polygynous societies practice some form of male
genital mutilation, and in societies in which wives
live in separate households that increases to 63%. [This would be skewed, depending
on the kind of statistical analysis, by the fact
that the vast majority of societies the cut male
genitals are Muslim.]
Only 14% of the monogamous societies in the database
practice male genital mutilation.
It might also be the case that selection works at a
group level, so that societies that enforce mutilation
are more stable because of less conflict over
paternity, Wilson says.
David Barash, an evolutionary biologist at the
University of Washington in Seattle, US, says that the
paper makes a convincing case.
...
Journal reference: Evolution and Human Behavior (vol
29 p 149)
|
Evolution & Human
Behaviour, May 2008, Vol 29, Issue 3,
pp 149-164
Male genital mutilation: an adaptation
to sexual conflict
Christopher G. Wilson
Abstract
Male genital mutilation (MGM) takes several
forms and occurs in about 25% of societies.
This behavior has puzzled anthropologists,
doctors and theologians for centuries, and
presents an evolutionary challenge since it
involves dangerous and costly surgery. I
suggest that MGM is likely to reduce
insemination efficiency, reducing a man's
capacity for extra-pair fertilizations by
impairing sperm competition. MGM may
therefore represent a hard-to-fake signal of
a man's reduced ability to challenge the
paternity of older men who are already
married. Men who display this signal of
sexual obedience may gain social benefits if
married men are selected to offer social
trust and investment preferentially to peers
who are less threatening to their paternity.
Clitoridectomy and vaginal infibulation
serve a parallel signaling function in
women, increasing a husband's paternity
certainty and garnering his increased
investment. Especially in societies where
paternity uncertainty and reproductive
conflict are high, the social benefits of
MGM as a signal may outweigh its costs. This
‘sexual conflict’ hypothesis predicts that
MGM should be associated with polygyny,
particularly when co-wives reside far apart,
and that MGM should reduce the frequency of
extramarital sex. MGM rituals should
facilitate access to social benefits; they
should be highly public, watched mainly by
men, and performed by a nonrelative. I found
support for these six predictions in two
cross-cultural samples. I also examined an
alternative hypothesis suggesting that MGM
signals group commitment for collective
action, particularly inter-societal warfare.
Although other forms of male scarification
fit this model, the distribution of MGM is
not predicted by frequency of inter-societal
warfare.
|
|
Gordon Gallup et al. put forward a theory that the
shape of the glans has evolved with the function of pumping a
rival's sperm out of the vagina, tending to ensure that a child
born after that intercourse is that of the man concerned and not
an earlier one. Their widely-quoted study does not mention the foreskin. One of
the popularisers of that theory, Jesse Bering, put readers' questions to Gallup for
Scientific American (May 30, 2009) about that issue.
|
READERS: The latex genitalia study wasn't terribly
convincing because the models were circumcised, and in
real life the foreskin would interfere with the
semen-displacing functions of the coronal ridge. So,
does the foreskin pose a problem for the semen
displacement theory?
GALLUP: The length of the foreskin is one of the most
variable features of the human penis. When most
uncircumcised males achieve an erection it pulls the
foreskin back over the glans and back down the shaft of
the penis, enabling the coronal ridge to do its business
and scoop rival males’ semen away from the woman’s
cervix. [It may also serve as
a "gasket", retaining semen, contradicting
the sperm displacement theory.] Because
circumcision reduces the diameter of the shaft
immediately behind the glans and accentuates the coronal
ridge, we’ve speculated that the practice of
circumcision may have unwittingly modified the penis in
ways that enable it to function as a more effective
semen displacement device. Armchair speculation? No. The
idea could be tested by comparing the incidence of
non-paternity between circumcised and intact males. My
prediction would be that circumcised males ought to
experience a lower incidence of being cuckolded.
READERS: So why did human penises evolve to have
foreskin at all then?
GALLUP: Evolution does not occur by design. The best
way to think about most adaptations is in terms of
cost/benefit ratios. I suspect that the foreskin
provided protection of the glans and what you see is the
result of a statistical compromise of sorts.
|
Meta-science
|
A dire power
Meta-analyses appear to be the ideal subject of
scientific debate - by combining dozens or hundreds
of previous studies, they allow us to have a truly
massive set of trials to work our statistics on, and
at the same time seem to offer balance in so far as
irregularly positive studies are often balanced out by
uncharacteristically negative ones. However, there is
a dire power within a meta-analysis, secretly wielded
by the author, and it is this highly subjective aspect
that lends each analysis its unique end result.
Put simply, the author gets to weigh how much an
experiment counts to the aggregate through his
evaluation of its quality. ... In other words, if you
want a study to count less, you tend to find more
flaws with it, and if you want it to count more, you
tend to gloss over flaws that might exist. In a normal
study, this power would wreak comparatively minor
havoc, because the trial number is low enough that a
modest result doesn't lead to massive
odds-against-chance numbers. However, when you
exercise this power with millions of pieces of data,
the impact is colossal ...
Dale DeBakcsy, "When Big Evidence
Isn't: The Statistical Pitfalls of Dean Radin's Supernormal"
Skeptical Inquirer, January-February, 2014
|
|
J. Sex Med.2013 Aug 12. doi:
10.1111/jsm.12293. [Epub ahead of print]
Does male circumcision affect sexual function,
sensitivity, or satisfaction?-A systematic review.
by Morris BJ and Krieger JN.
ABSTRACT
Introduction
Circumcision of males is commonly carried out
worldwide for reasons of health, medical need,
esthetics, tradition, or religion. Whether
circumcision impairs or improves male sexual function
or pleasure is controversial.
Aims.
The study aims to conduct a systematic review of the
scientific literature.
Methods
A systematic review of published articles retrieved
using keyword searches of the PubMed, EMBASE, and
Cochrane databases was performed.
Main Outcome Measures
The main outcome measure is the assessment of findings
in publications reporting original data relevant to
the search terms and rating of quality of each study
based on established criteria.
Results
Searches identified 2,675 publications describing the
effects of male circumcision on aspects of male sexual
function, sensitivity, sensation, or satisfaction. Of
these, 36 met our inclusion criteria of containing
original data.
Those studies reported a total of 40,473 men,
including 19,542 uncircumcised and 20,931 circumcised.
Rated by the Scottish Intercollegiate Guidelines
Network grading system, 2 were 1++ (high quality
randomized controlled trials) and 34 were case-control
or cohort studies (11 high quality: 2++; 10
well-conducted: 2+; 13 low quality: 2-). The 1++ ,
2++, and 2+ studies uniformly found that circumcision
had no overall adverse effect on penile sensitivity,
sexual arousal, sexual sensation, erectile function,
premature ejaculation, ejaculatory latency, orgasm
difficulties, sexual satisfaction, pleasure, or pain
during penetration. Support for these conclusions was
provided by a meta-analysis.
Impairment in one or more parameters was reported in
10 of the 13 studies rated as 2-. These lower-quality
studies contained flaws in study design (11),
selection of cases and/or controls (5), statistical
analysis (4), and/or data interpretation (6); five had
multiple problems.
Conclusion
The highest-quality studies suggest that medical male
circumcision has no adverse effect on sexual function,
sensitivity, sexual sensation, or satisfaction.
|
|
News Flash! Circumcision advocates advocate
circumcision!
Circumcision advocates Brian Morris and John
Krieger's "meta-analysis" (annotated version here)
compounds the faults of the above studies.
- They rank the ill-defined and circumcision-driven
Masters and
Johnson "study", never peer-reviewed or
published in a scientific journal, as "2++ (high
quality)".
- They review a
Kenyan study in detail, entirely uncritically,
though one of them is a co-author.
- They refer to their own critiques of studies that
find detriments of circumcision, without reference
to rebuttal of those critiques.
- Several of the studies cited provide no data on
sexual satisfaction.
- They unfailingly mark down all studies finding
detriment to circumcision and mark up all those
finding benefit.
Professor Morris has a
track record of statements that do not correspond with
the facts.
|
Sexual
Medicine,
23 April 2015, https://doi.org/10.1002/sm2.67
Histological Correlates of Penile
Sexual Sensation: Does Circumcision Make a
Difference?
Guy Cox MA, DPhil, John N. Krieger MD, Brian J.
Morris DSc, PhD
Abstract
Introduction
The question of whether removal of sensory receptors
in the prepuce by circumcision affects sensitivity
and/or sexual pleasure is often debated.
Aims
To examine histological correlates relevant to penile
sensitivity and sexual pleasure.
Methods
Systematic review of the scientific literature on
penile structures that might affect sensitivity and
sexual sensation. Articles were included if they
contained original data on human male penile histology
or anatomy. Individual articles, including reference
lists, were evaluated. They were then considered in
relation to physiological data from articles retrieved
by a previous systematic review.
Results
We retrieved 41 publications on penile structure.
Considered in the light of 12 reporting physiological
measurements, our evaluation finds that sexual
response is unlikely to involve Meissner's corpuscles,
whose density in the prepuce diminishes at the time of
life when male sexual activity is increasing. Free
nerve endings also show no correlation with sexual
response. Because tactile sensitivity of the glans
decreases with sexual arousal, it is unrelated to
sexual sensation. [This does
not follow.] Thermal sensitivity seems
part of the reward mechanism of intercourse.
Vibrational sensitivity is not related to circumcision
status. Observations that penile sexual sensation is
higher [immdiately, but not
long-term] post circumcision are
consistent with greater access of genital corpuscles
to sexual stimuli after removal of the prepuce. This
is based on the distribution of these corpuscles
(which are located in the glans) and, in uncircumcised
men, the position of the retracted prepuce during
intercourse, rather than any change in the number of
genital corpuscles. The scientific literature suggests
that any sexual effect of circumcised men may depend
solely on exposure of the glans and not on the absence
of the prepuce.
Conclusion
Based on histological findings and correlates of
sexual function, loss of the prepuce by circumcision
would appear to have no adverse effect on sexual
pleasure. Our evaluation supports overall findings
from physiological measurements and survey data.
This study is remarkable. It is as
if three blind men were trying to study the role of
the eyes in the sense of sight.
The body of the article contains
these remarkable passages:
... many studies, beginning with Masters and Johnson 10, have
attempted to measure penile sensitivity of circumcised
and uncircumcised men via a range of techniques (see
recent review: 11). ...
Masters and Johnson compared the tactile sensitivity of
the glans in circumcised and uncircumcised men 10 and found no
difference. It was admittedly a
crude test, and no statistics were given.
-
10
Masters
WH, Johnson VE.
Human Sexual Response.
Boston:
Little Brown; 1966.
-
11
Morris
BJ, Krieger JN.
Does male
circumcision affect sexual function,
sensitivity or satisfaction?—A systematic
review. J
Sex Med 2013;10:2644–2657.
The references to the foreskin and genital cutting in
Masters & Johnson's book is dissected earlier
on this page. In brief, its ignorance of the
foreskin and cultural bias towards cutting is blatent.
But what is stranger still, Morris and Krieger's "recent
review" (also critiqued above)
accords it "2++ (High quality case control ... studies
with a very low risk of confounding or bias and a high
probability that the relationship is causal)" status!
|
Work in progress
Some experiments are underway, using anaesthetics to remove
sensation from the foreskin but not the glans, or the glans but
not the foreskin:
|
"Ken McGrath, senior lecturer of pathology at
Auckland University of Technology...an internationally
recognised researcher on the effects of
circumcision...recently simulated circumcision by
anaesthetising his foreskin. He describes it as a
disturbing experience, going from full sensitivity to
almost none."
"Foreskin's
Lament"
Sunday Star-Times
(New Zealand)
July 29,2001
|
Other measurements of tactile sensitivity - those that Masters
and Johnson and Melman et al. ought
to have done - are now being made. They may further clarify the
role of the foreskin in sex.
Evidence is growing that intact men's arousal is more graduated
- that orgasm comes less suddenly and hence is more
controllable. This can be predicted from the possession of more
nerve endings - a volume control, not just a switch, for sexual
feelings.
Male
and female sexual anatomy
- closer than we thought?
Intactivists have been inclined to suppose that male
and female genitalia are differently innervated - the
clitoris apparently being richly endowed with nerves
compared to the glans penis - and it has been assumed
that the clitoral prepuce, the woman's equivalent to a
foreskin, is correspondingly nerveless. (This, in
part, gives rise to the failure to communicate between
opponents of FGM and of MGM.)
However, one women's experience suggests that that is
not the case and that a woman's "foreskin" is as
sensitive as a man's:
In myself, I have ... encountered what would be the
inner layer of foreskin (that rests against the
glans). If a woman's clitoral hood is properly
pulled back, a very distinct line of demarcation,
separating the inner foreskin from the outer
non-sensitive skin, is quite visible. Stimulation of
this "inner foreskin" gives me greater pleasure than
just direct glans stimulation.
I have read that without the foreskin, men do not
have a warning system to tell them when orgasm is
imminent. I believe that women have the same
reaction. When I can stimulate the "inner foreskin"
of my clitoral hood, the sensations are much
different, more intense, than if I do not stimulate
it. And when I do not, I, as a woman, also get the
"orgasm sneaking up" problem. I think this may well
be because of a lack of triggers, much like a
circumcised man.
Also, the pliability of the skin allows for more
variation in masturbation technique, like an uncut
man also gets to employ. I can cover or uncover at
my will, when I feel the need; this liberty that I
take for granted has been denied millions of men.
- Private communication
If this is true, it is obscured by the (generally
agreed) fact that women's sexual response is more
"global" and less centred on the genitalia than men's,
|
Resources
One of the few sex guides available in the US that assumes the
male to be intact is The
Guide
to Getting It On! (The Universe's Coolest and Most
Informative Book About Sex) by Paul Joannides, illustrated by
Daerick Gross, available from Amazon.com, where the first eight
reviews have all rated it five stars

An instant classic when it first came out in 1972, "The Joy of
Sex" by Alex Comfort, illustrated with drawings by Charles
Raymond and Christopher Foss, Modset Securities Ltd/Quartet
Books Ltd (London), was more or less pro-foreskin
| foreskin |
Cutting off this
structure...persists - on the ground ...
either that cancer
of the cervix and penis
is rarer when it is done (washing probably
works as well) or that it slows down orgasm
(for which there is no evidence). We're
against it, though for some it is already too
late. 'To cut off the uppermost skin of the
secret parts', says Dr. Bulwer, 'is directly
against the honesty of nature, and an
injurious insufferable trick put upon her.'
p
65 (1974)
|
|
and illustrated mainly with intact men. The latest edition,
The New Joy of Sex (The Joy of Sex Series) by Alex Comfort,
edited by Julie Rubenstein, photographs by Clare Park. now
attracts mainly negative reviews at Amazon.com for its
old-fashioned attitudes.

Offsite: an intact Briton with a US wife has written a page for
women about how
to please an intact man. He generalises from himself, is a
bit shaky on his anatomy, and presents a rather alarming
metallic analogy, but has a detailed chart of what gives
pleasure.
Related pages:
HOME
|
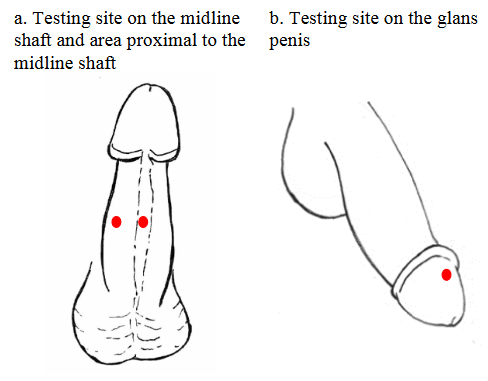
![Bossio - test site on the [outside of the] foreskin](Images/sex-bossio-testing-site.png)

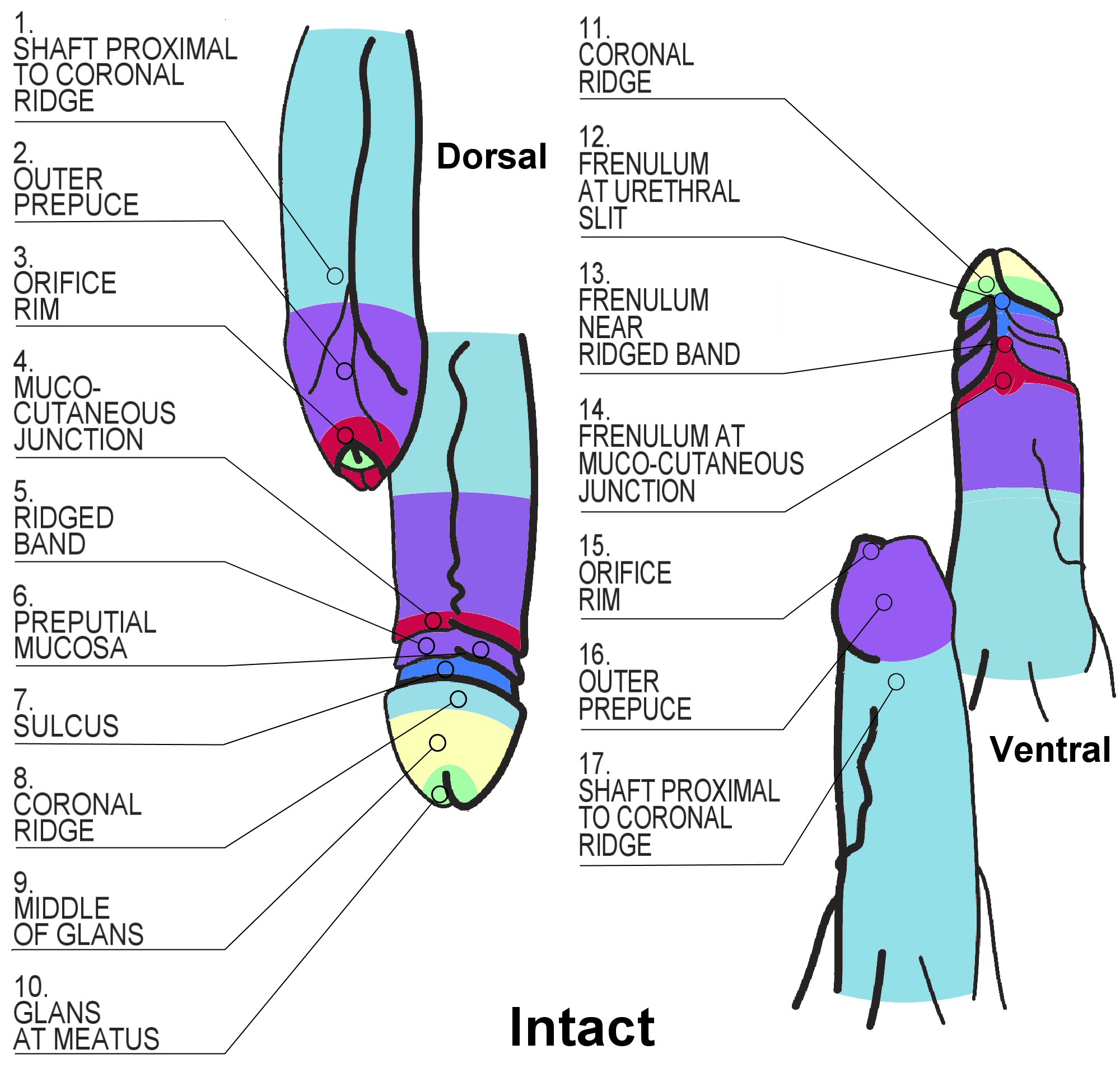{kind=link}
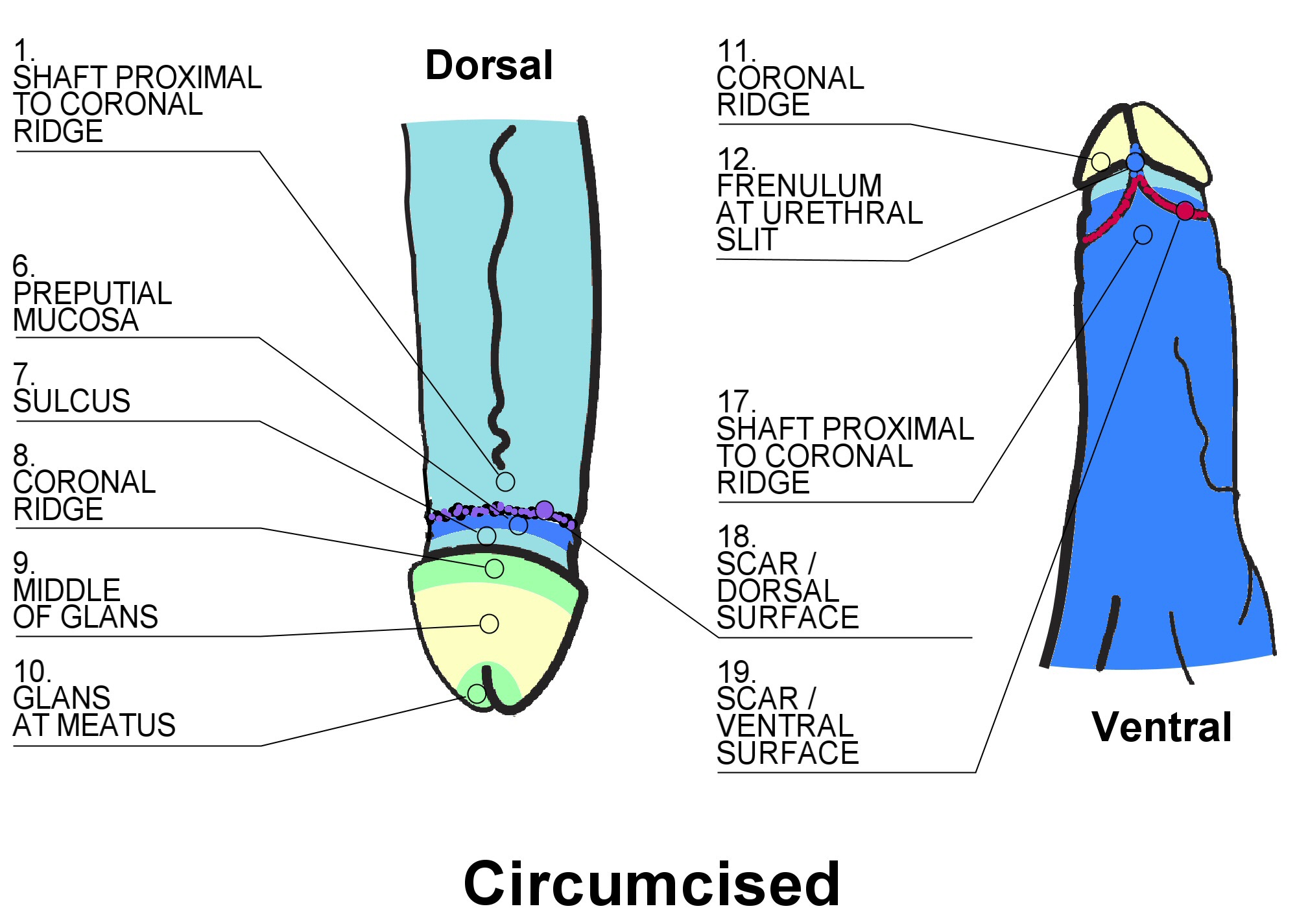{kind=link}
{kind=link}