This page used to begin "Circumcision never causes death
directly, of course - how could it?" but in January 2007 a
boy died in London apparently from shock directly caused
by his circumcision.
Circumcision can cause death indirectly in a variety of ways,
such that if the baby had not been circumcised, he would not
have died. Below are cases of death caused by:
Invariably, the indirect, involuntary cause is given all the
blame, and the decision to circumcise, none. So circumcision
continues to be promoted as "safe" and babies continue to die. The suicide of David Reimer
after a ruined life was ultimately due to his botched,
unnecessary circumcision.
The actual rate of death from "medical" circumcision is
unknown. A rate can be calculated from Gairdner's
paper of one death in 5600 circumcisions, but that was in
England in the 1940s, and it must be lower now. Grimes
(1978) gave a figure of two deaths per million, but citing a
1953 study. A Brazilian study finds a
rate of one death in 7692 circumcisions. It is certainly more
than one in 1,200,000 since there is on average more than one in
the US every year. The problem is that deaths indirectly due to
circumcision, such as that of Dustin Evans Jr,
are not attributed to it as they should be, since it is
unnecessary surgery. (If it were necessary, the death could be
ultimately blamed on the condition that made it necessary.)
THYMOS: Journal of Boyhood Studies, Vol. 4,
No. 1, Spring 2010, 78-90
LOST BOYS: AN ESTIMATE OF U.S.
CIRCUMCISION-RELATED INFANT DEATHS
- Dan Bollinger
Abstract: Baby boys can and do succumb as a result of
having their foreskin removed. Circumcision-related
mortality rates are not known with certainty; this
study estimates the scale of this problem. This
study
finds that approximately 117 neonatal
circumcision-related deaths (9.01/100,000) occur
annually in the United States, about 1.3% of
male neonatal deaths from all causes. Because infant
circumcision is elective, all of these deaths are
avoidable. This study also identifies reasons why
accurate data on these deaths are not available, some
of the obstacles to preventing these deaths, and some
solutions to overcome them.
Serious and Fatal Complications after Neonatal
Circumcision
Annette Schröder, Walid A. Farhat, David Chiasson,
Gregory J. Wilson, Martin A. Koyle
Published:December 29,
2021DOI:https://doi.org/10.1016/j.euf.2021.12.005
Abstract
Neonatal circumcision (NNC) is the most frequently
performed surgical procedure worldwide and is generally
considered safe in Western societies. Deaths attributed
to NNC are seldom reported and are mostly explained by
lack of adherence to medical standards. We reviewed our
emergency department database for circumcision-related
emergency admissions. During 2000–2013, 19 previously
healthy neonates were admitted for acute complications
after circumcision. Four were admitted for bleeding,
with hemophilia identified in two cases and von
Willebrand disease in one. Eight boys required emergency
surgery, three for severe bleeding. Four boys with
amputation of the glans underwent immediate surgical
reconstruction. One infant was taken to the operating
room to remove an obstructing Plastibell ring. Seven
boys were admitted to the intensive care unit with
severe bleeding or sepsis, three of whom ultimately
progressed to hemorrhagic or septic shock. Two of these
children died of their complications. We estimate that
the annual incidence of severe complications requiring
hospitalization after NNC in the Greater Toronto Area
was approximately 0.01% [1
in 10,000], and the incidence of fatalities
over the 14-yr review period was approximately 0.0012% [1 in 83,000]. Our
results indicate that the risk of serious complications
and death as a result of NNC is greater
than generally assumed.
[Extrapolating from a
small number of complications and deaths at one
hospital to the total for a country or the world is
subject to the possibility of a large error.]
A significant number of youths die from infection after tribal
circumcision every year in Africa
An average of 39 a year (80 in 2009) in Eastern Cape province
alone.
Ryleigh McWillis - death from blood loss
AUTOPSY
FINDINGS
...
MEDICAL CAUSE OF DEATH
(1) Immediate cause of death: a) Multi-organ
ischemia, due to or as a consequence of b)
exsangination [loss of blood],
due to or as a consequence of c)
circumcision
(2) Other significant conditions contributing to
death: Post-surgical exsanguination
Classification of the event: Accidental
Date signed: 19 January 2004
T.E. Chico Newell, Coroner
[The evidence would justify
classifying Ryleigh's death as Iatrogenic
and recommending that circumcision of infants be
removed from the category of elective procedures.]
THE DADE COUNTRY MEDICAL EXAMINER DEPARTMENT,
Miami, Florida
Name....MANKER,.Demetrius.....June.23,1993....11:00am.........Case
No. 93-1711
EXTERNAL EXAMINATION:
The body is that of a 25-1/2 inch, 15
pound, very pale appearing Negro male appearing
consistent with the stated age of 6 months. ... No
anomalies are evident.
When initially viewed, a large amount of
congealed blood covers the head of the penis. Removal
of this disclosed a circumcision site that appears
unremarkable along the dorsal surface of the penis.
Ventrally, however, a gaping defect of approximately
12 x 14 millimeters is evident with a large amount of
extravasated blood in the subcutaneous tissues
extending along the shaft of the penis nearly to the
scrotal sac.
...
CAUSE OF DEATH: Exsanguination DUE TO: Penile Circumcision
[signed]
Charles V. Wetli, M.D.
Deputy Chief Medical Examiner
In this case, unlike the one above, the cause of
death is correctly attributed, yet there is no record
of any further action being taken.
Joshua Haskins - weakened by a heart condition
Jill and Shane Haskins' baby Joshua was born on
August 16, 2010 with a major heart defect (Hypoplastic
Left Heart Syndrome, HLHS). He had heart surgery at 3 days old, and
was circumcised on October 5, 2010. He died on October
6.
Jill blogged and accepted comments
before, during and after the birth, surgery,
circumcision and death. (Most strikingly, she blogged
after the circumcision, while Joshua was still
struggling against haemorrhage, "I Almost Killed My
Son". Her blog now contains no reference to
circumcision.)
Nobody will ever be able to say with certainty that
Joshua would have lived if he had not been
circumcised. The doctors insisted that his
circumcision had nothing to do with it, but they would
say that, wouldn't they? What we can say (and even Amy
Tuteur admits) is that circumcising him could not have
helped. For the doctors to go ahead with the surgery
in his weakened condition does illustrate the
compulsion to circumcise that has been called the
Toxic Circumcision Culture.
On Radio KQED on August 29 2012,
the ethicist for the American Academy of
Pediatrics, Dr Douglas Diekema, grossly misstated the
case (starting at 12:40):
"There's at least, y'know, one of these
cases that gets trotted out, involved a very
sick baby that was likely to die anyway, and
his parents wanted him circumcised before,
ah, his death, and to attribute that to a
circumcision is silly, um, that kind of a
death."
His mother's blogs give the lie to that
interpretation.
Brayden Tyler Frazier - blood-loss
March 8, 2013
Another circumcision death
An 11-day-old boy has died died at UC Davis
Children's Hospital in Sacramento, California, two
days after being circumcised in the nearby town of
Lodi.
According to his grandfather, Brayden Tyler Frazier
had been taken to the doctor when he was a week old
because he had been sleeping constantly and not
eating. His parents had also noticed that his neonatal
sticks and pricks had not healed quickly, and had to
stay bandaged for two days or more.
The doctor in Lodi sent them home with instructions
to monitor his condition and after two days, he was
circumcised. It was later discovered that the wound
had continued to bleed. He was taken back to the
doctor, then to Urgent Care, then to the ER, and then
transferred to UC Davis Medical.
He had "generalized bleeding" and an unidentified
infection.
Over the two days after his circumcision, he went
into seizures and a coma, and died.
It was claimed online that the baby should have been
tested for haemophilia, but a paediatric
haematologist/oncologist comments
Coagulation studies are not routinely done
before many types of surgeries, including
circumcisions. ...
Also, coagulation studies are not a part of
routine newborn screening tests.
Coagulation is complex, and involves the
platelet cell and a couple dozen chemicals /
proteins, to clot when needed but also not
to clot in inappropriate locations, or
excessively, and to additionally reabsorb
clots after they have done their jobs.
Plus hemophilia isn't a single disorder;
there are two main types of "hemophilia"
(deficiency of Factor 8 or Factor 9 ). But
there are many other reasons to bleed
excessively. However, a combination of
several functional tests can narrow down the
list of specific aspects of the coagulation
system that need testing, in a given
individual whose screening functional tests
are abnormal, in order to identify what
needs to be done to treat that individual's
bleeding/risk.
However it is more complicated in newborns:
1) Of the couple dozen chemicals, many are
in different levels in newborns. For several
reasons, some aspects of the newborn's
system are hypo-coagulable [blood won't
clot] while others are hyper-coagulable
[blood clots very easily] and it generally
balances out. So there are different normal
ranges for results in infants.
2) Most tests of the coagulation system
involve drawing blood from a vein or artery
and simultaneously mixing it with
anticoagulants (different anticoagulants for
different tests). These tests also involve a
relatively large amount of blood.
Additionally the tissue factors, that
trigger the initiation of the clotting
system in injuries, are released from a heel
stick and affect clotting studies.
3) It is however easy to do extensive or
specific coagulation tests in newborns.
When planned, the blood is correctly drawn
at delivery from the umbilical cord, taking
the blood otherwise left in the placenta...
This can be planned when a family history
[of haemophila] is present or there are
other reasons to test.
Surgeries / procedures that have no medical
necessity, [such as] circumcision, should
not be done.
- on Brother K's Facebook page, Octorber
5, 2018
She comments that this happened in 2013,
and that the rabbi no longer performs britot
and has become an Intactivist.
Dustin Evans Jr. - death from anaesthetic
Dustin Evans Jr was born in Cleveland, Ohio in
October 1998. He was circumcised by a Dr Russell soon
after, who took so much shaft skin that the scar
healed as a wideband stricture (a tight "collar")
around his penis, preventing him from urinating. When
he was given sevoflourane, an anaesthetic, in order to
"revise" his circumcision, he immediately died of
cardiopulmonary arrest.
His father said, "You think, 'What
could go wrong with a circumcision?' The next
thing I know, he's dead."
Oddly, the report of Cuyahoga County Coroner,
Elizabeth Balraj MD, says
IDENTIFYING MARKS AND SCARS:
None
EVIDENCE OF RECENT THERAPY: [does not
mention his circumcision]
EVIDENCE OF RECENT INJURY: None
A
FAMILY doctor who killed a nine-year-old boy by
giving him a massive overdose of a pain-killing drug
during a circumcision operation, was given a
one-year suspended jail sentence yesterday. Dr.
Mahbubul Alam, 59, of Handsworth Wood, Birmingham,
admitted the manslaughter in July 1991 of Raju Miah,
of Smethwick, who died in hospital six days after
being given diamorphine (heroin).
Timothy
Barnes QC, for the prosecution, told Stafford Crown
Court that the boy was taken for the operation by
his grandfather. Dr. Alam, who had performed four
circumcisions that day, administered 10mg of
diamorphine, "five to six times the appropriate
dose."
Mr.
Barnes said: "Raju was given 10mg of diamorphine,
which sedates the brain and also tends to depress
breathing. After the operation the boy was still
unconscious and when he was driven back to the
family home, Dr. Alam tried to arouse him by
sprinkling water on his face and lightly smacking
his face." He said shortly after the doctor left,
the boy's condition worsened and he was taken by
ambulance to hospital. After six days, he was
certified brain dead and the life-support machine
was switched off.
Mr.
Barnes said the cause of death was narcotic
poisoning. "The choice of drug was wholly
inappropriate and on a boy of his age was grossly
negligent," he said. Mr. Justice Buckley said: "I
only hope Raju's family can find it in their hearts
that sending Dr. Alam to prison...would serve no
public interest and do nothing good for the memory
of Raju."
Body of 9-Week-Old Infant
Allegedly Found Dead; Parents Under Custody
by Regina Inonog
The Sarasota County Sheriff’s
Office has recovered the body of an infant believed to
be ... Chance Walsh ... in North Port, Florida. ...
Chance, who was only 9 weeks old, was first reported
to be missing a month ago ... [Chance's mother,
Kristen] Bury’s stepmother, Kimberly Millwater. said
that ... Bury told her ... she “despised Chance ...
because he wasn’t Duane.”
[Kristen] Bury gave birth to Duane Jacob Walsh on March
13, 2014, only for paramedics to find him dead 22 days
later. Medical examiners found out that Duane
died of a kidney infection that resulted from a
botched circumcision.
[So cutting one baby may be
said to have caused two deaths.]
A child was born without incident in a West Virginia
hospital and was circumcised before discharge. Two
days later, the baby boy was brought to a health
center where the doctor did a follow-up examination.
Four days after that, the child was rushed to a
hospital emergency room after developing a fever and
undergoing seizures. The ER physician telephoned the
doctor who had performed the circumcision and decided
not to admit the child. The next morning, the mother
brought the infant back to the ER where he suffered
more seizures and was noted to have a greenish cast to
the penis. That afternoon the child was transferred to
a medical center, where he died 4 hours later.
The cause of death was found to be septicemia derived
from an infection secondary to the circumcision. Both
physicians were sued for negligence for failure to
admit the child to the hospital on the first visit to
the ER. After 6 months, a settlement of $150,000 was
reached.
Paediatric Death Review Committee:
Office of the Chief Coroner of Ontario
A male infant at 37 weeks' gestation was born ...
weighing 3.9 kg, with Apgar scores of seven at 1 min
and nine at 5 min, Prenatally mild bilateral
dilation of renal pelvises and ureters was noted on
ultrasound. A urology consultation at 36 weeks'
gestation suggested a possible normal variant ...
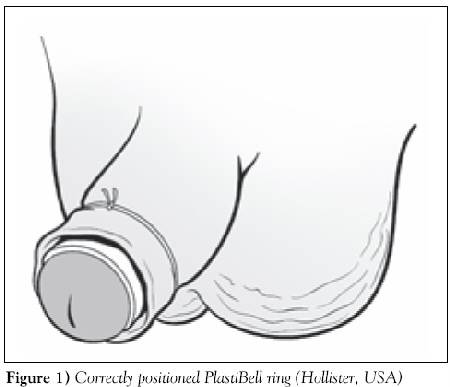
The baby was bottle-fed and was reported to he
doing well when he was circumcised using a PlastiBell
ring (Hollister, USA) at 10:00 on the seventh day of
life (Figure 1).
Local anaesthetic was not used. Some slight oozing
was noted during the procedure but it was not a
problem at discharge.
Five hours later, the parents returned to their
family doctor with the infant, reporting that he
was very irritable and had blue discolouration below
the umbilicus [navel] when he cried. The doctor
confirmed this observation and noted that the penis
was slightly swollen. ... He had several loose
stools, and it could not be determined with
certainty whether he had voided [emptied his
bladder]. ...The baby was subsequently discharged
home.
The infant was brought to a different hospital 14 h
after the circumcision. He was now noted to be
extremely irritable, with marked swelling of the
penis and with marked swelling and cyanosis
[blueness] of the scrotum and perineum [region
behind the scrotum]. He had grunting respirations
and was cyanotic below the umbilicus ... He was
transferred to a tertiary care centre, where the
bladder was identified as being distended to the
level of the umbilicus, The PlastiBell ring was
removed 16 h after the circumcision and a catheter
was passed. The bladder was drained and the bluish
coloration below the umbilicus subsided. Urine
volume was not recorded. Over the next few hours,
the infant went into septic shock with purpura
fulminans, and went on to develop multiorgan
failure and disseminated
intravascular
coagulopathy [a state of increased propensity
for blood-clot formation] ... He died seven days
after his circumcision from hypoxic-ischemic
encephalopathy [damage to cells in the brain
and spinal cord from getting too little oxygen]. ...
Complications of meatal obstruction [blockage of
the urinary opening of the glans]
with the PlastiBell technique have been previously
described in the literature (1,2). Necrotizing
fasciitis as a complication of circumcision
is rare, and all cases reported seem to be
associated with the PlastiBell technique (2,3) The
finding of cyanosis below the umbilicus after
circumcision due to meatal obstruction caused by a
misplaced PlastiBell ring resulting in bladder
distension and obstruction of venous return has also
recently been described (1). A review of
circumcision complications suggest that these may
occur mote frequently than is conventionally
believed (2,4)
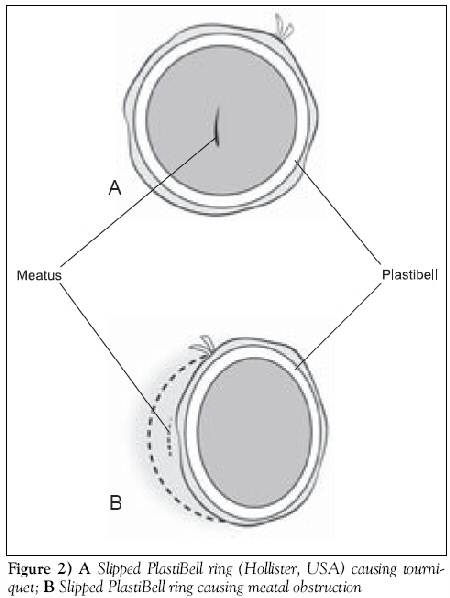
The members of the Paediatric Death Review
Committee of the Office of the Chief Coroner of
Ontario were collectively aware of complications
from their own institutions, including two children
with necrosis of the glans, two infants requiring
transfusion, one infant with a buried penis
secondary to circumcision, numerous cases of
retention of a PlastiBell ring, one infant with a
slipped PlastiBell ring causing a penile tourniquet,
and one infant with meatal obstruction due to a
misplaced PlastiBell ring (Figures 2A and 2B).
None of these complications were reported in the
medical literature and are therefore not available
in a retrospective literature review. It is
concerning that none of the initial three
physicians who saw this infant, including the
physician who performed the procedure, identified
this problem as a meatal obstruction, although they
were all concerned about, a possible link with the
recent circumcision.
In this infant, there was no description of the
glans by the physician removing the PlastiBeil ring.
If the foreskin is pulled too tight, then there will
be considerable tension pulling the ring against the
glans, thus compressing the urethra and making
urination difficult or impossible. This is the
mechanism described in the case report by Ly and
Sankaran (I) We propose the mechanism shown in
Figure 2B, given the rapid onset of symptoms,
suggesting a complete obstruction. These coukl be
differentiated clinically. In Figure 2A, the meatus
would be visible in the middle of the ring and a
catheter would be difficult or impossible to pass.
In Figure 2B, the meatus would not be visible. The
management of both complications would be the
immediate removal of the PlastiBell ring. Perhaps a
prospective surveillance study by the Canadian
Paediatric Society of the complications of
circumcision is warranted. Such a study would
provide more accurate information for the ethical
requirement of informed consent.
[Perhaps a ban on
non-therautic neonatal circumcisions by members
of the Canadian Paediatric Society is warranted.
As the headline implies, this is not a
minor procedure.]
In reply to a complaint, the College of Physicians
and Surgeons of Ontario completely exonerated the
doctor. In fact so excellent did they make his work
seem, you would think the baby was still alive.
...The Paediatric Death Review Committee felt
that Baby A had a urethral meatal obstruction
secondary to the Plastibell ring, which it noted was
not a common complication. They questioned whether
the family physician who performed the circumcision
was aware of this potential complication....
...Dr. X ... did not believe there was anything
he/she could have done differently. When he/she
examined the infant when the parents returned
later in the day, there was no meatal obstruction.
...
he/she had tried using local anaesthetic over
the years but found that the infant appeard to
be in just as much pain, if not more
the needle to inject the anaesthetic is very
painful, as is the local anaesthetic itself
there is a concern about the increased chance
of infection with the injecting of local
anaesthetic, as the puncture holes from the
needle would be in the diaper area surrounded by
urine and faeces, below the area of the
circumcision [...which
raises questions about the risk of infection
at the much bigger circumcision wound
itself...]
there is a concern regarding potential
allergic reaction to the anaesthetic
local anaesthetic tends to distort the site of
the circumcision and make it more difficult to
perform
the period of restraint for the infant in the
cirucmsion board is prolonged when using local
anaesthetic, and the restraint causes the infant
distress
in the community, local anaesthetic is not
used, and not the standard of care
[This will all be of
interest to parents who assume that circumcision
is made painless nowadays.]
...it is not possible to determine with any
certainty how the urethral meatus became
obstructed by the Plastibell device. ...
Committee's final comments
The Committee has the utmost sympathy for the
parents of Baby A, given the very tragic outcome
in this case. However, we are satisfied that the
care provided by Dr. X in this case was
conscientious and appropriate, and in compliance
with the relevant legal and ethical standards in
place at the time the circumcision was performed.
[THEN WHY IS THE CHILD
DEAD?]
DISPOSITION
... no further action will be taken with respect
to this matter.
Circumcisions for medical reasons in the Brazilian
public health system: epidemiology and trends.
Korkes F, Silva Ii JL Pompeo AC
Abstract
OBJECTIVE:
To evaluate the epidemiological factors associated to
medical circumcision, based on data from the Brazilian
public health system.
METHODS: Using the Unified Health System
public database between 1984 and 2010, hospital
admissions associated with surgical treatment of
phimosis were searched. A total of 668,818 men
admitted to public hospitals who underwent
circumcision were identified and included in the
present study.
RESULTS:
A mean±standard deviation of 47.8±13.4
circumcisions/100,000 men/year was performed through
the Unified Health System for medical reasons. During
the 27-year period evaluated, 1.3%
of the male population required circumcision for
medical reasons. [So
98.7%
of routine circumcisions are wasted on boys and
men who will never need it.] Total
number of circumcisions and circumcision rate
increased in childhood, declined progressively after 5
years of age and rose again progressively after the
sixth decade of life. In the regions of the country
with better access to healthcare, 5.8% of boys aged 1
to 9 years old required circumcisions. [Or
were circumcised whether they needed it or not.]
From 1992 to 2010 there were 63
deaths associated with circumcisions (mortality rate
of 0.013%).
[That's one death in 7692
circumcisions. In this USA, that would amount to 156
circumcision deaths per year.]
CONCLUSION:
In conclusion, yearly circumcision rates could be
estimated in Brazil, and a very low mortality rate was
associated with this procedures. Circumcision is
mostly performed in children in the first decade of
life and a second peak of incidence of penile foreskin
diseases occurs after the sixth decade of life, when
circumcision is progressively performed again.
[This study was circulated
by Prof. Brian Morris, who presumably thinks this
is an "acceptable" death rate.]
Death by circumcision, in South Africa a regular event
Male circumcision morbidity and mortality
statistics
Eastern Cape, South Africa, 2001-5
Neonatal circumcision and prematurity are
associated with sudden infant death syndrome
(SIDS)
Eran Elhaik
ABSTRACT
Background: Sudden Infant Death Syndrome
(SIDS) is the most common cause of postneonatal
unexplained infant death. The allostatic load
hypothesis posits that SIDS
is the result of cumulative perinatal painful.
stressful, or traumatic exposures that tax
neonatal regulatory systems.
Aims: To test the predictions of the
allostatic load hypothesis we explored the
relationships between SIDS and two common
phenotypes, male neonatal circumcision (MNC) and
prematurity, Methods: We collated latitudinal data
from IS countries and 40 US states sampled during
2009 and 2013. We used linear regression analyses
and likelihood ratio tests to calculate the
association between SIDS and the phenotypes.
Results: SIDS
mortality rate was significantly and positively
correlated with MNC. Globally (weighted):
Increase of 0.6 (95% CI=0.01-0.1, t=2.86, p=0.01)
per 1000 live-births SIDS mortality per 10%
increase in circumcision rate. US (weighted):
Increase of 0.1 (95% CI=0.03-0.16. t=2.81, p=0.01)
per 1000 live-births unexplained mortality per 10%
increase in circumcision rate. US states in which
Medicaid covers MNC had significantly higher MNC
rates (X- =0.72 vs 0.49; p=0.007) and male/female
ratio of SIDS deaths (X- = 1.48 vs 1.125; p=O.015)
than other US states. Prematurity was also
significantly and positively correlated with MNC [sic: with SIDS?].
Globally: Increase of 0.5 (weighted: 95% Cl:
0.02-0.086, t=3.37. P =0.004) per 1000 SIDS
mortality per 10% increase in the prematurity
rates. US: Increase of 1.9 (weighted: 95% Cl:
0.06-0.32, t=3.13, p=0.004) per 1000 unexplained
mortalities per 10% increase in the prematurity
rates. Combined, the phenotypes increased the
likelihood of SIDS.
Conclusions: Epidemiological
analyses are useful to generate hypotheses but
cannot provide strong evidence of causality. Biological plausibility is
provided by a growing body of experimental and
clinical evidence linking aversive preterm and
early-life SIDS events. Together with
historical and anthropological evidence, our
findings emphasize the necessity of cohort studies
that consider these phenotypes with the aim of
improving the identification of at-risk infants
and reducing infant mortality.
Relevance for patients: Preterm birth and
neonatal circumcision are associated with a
greater risk of SIDS, and efforts
should be focused on reducing their rates.